Case Report
Open Access, Volume 3
Urachal Adenocarcinoma and Immunotherapy Treatment: Case Report from Palestine
Sami SM
University of Palestine, Palestine.
University of Palestine, Palestine.
Urachal cancer is a rare form of bladder cancer that arises from the urachus, a vestigial musculofibrous band that extends from the dome of the bladder to the umbilicus. Urachal cancer often presents at an advanced stage and has a dismal prognosis. We present a case of a woman with urachal cancer that recurred rapidly post-partial cystectomy. The patient was treated with chemotherapy regimens, including an oral antiangiogenic drug as part of a clinical trial. Our case illustrates the aggressive nature of this disease, the difficulty in accessing drugs for the treatment of rare cancers and the lack of late stage clinical trials to help guide therapeutic decisions.
Manuscript Information: Received: Jun 20, 2023; Accepted: Jul 19, 2023; Published: Jul 26, 2023
Correspondance: Sami SM, University of Palestine, Palestine. Email: sami_sm2006@yahoo.com
Citation: Sami SM. Urachal Adenocarcinoma and Immunotherapy Treatment: Case Report from Palestine. J Oncology. 2023; 3(2): 1098.
Copyright: © Sami SM 2023. Content published in the journal follows creative common attribution license.
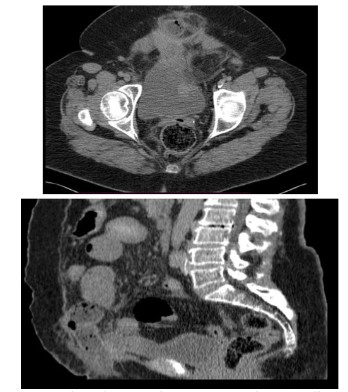
A 68-year-old female patient was in her usual state of health until April 2021, when she suddenly started to complain of diffuse colicky abdominal pain associated with abdominal distention and constipation. Patient sought medical advice where abdomen CT scan was done and showed midline lower abdominal wall hernia containing bowel loops causing small bowel obstruction (Figure 1).
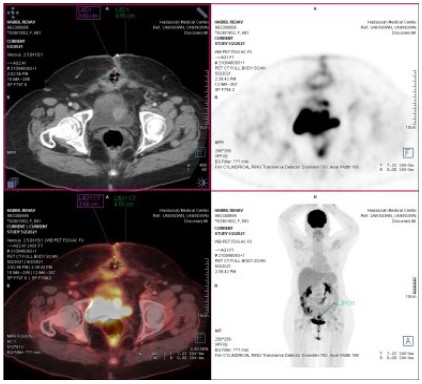
Urgent laparotomy was done and intraoperatively they found mass about 5 cm above the urinary bladder amalgated with terminal ileum invading and obstructing lumen, Limited resection with side-to-side anastomosis with hernia sac excision was done. After that pathology showed a moderately differentiated adenocarcinoma. Pathology also shows that the neoplastic cells are positive for CK7, CK20 (focal-faint), B-catenin (membranous) and CK-MNF116 immunostains, and they are negative for CDx2 immunostain. The immunohistochemical features were highly suggestive of urachal origin of the malignancy and exclude the possibility of being of lower GI origin. So that, patient was diagnosed as a case of urachal adenocarcinoma and the decision was to start patient on 5FU 200 mg D1-5. LCV 10MG/M MG D1-5, Cisplatin 20 MG/M D1-5, Gemcitaben 200 mg/m D1-5 as neo-adjuvant chemotherapy. On Aug. 2021 PET scan was done which was free and whole-body CT scan was done on October 2021 which showed no evidence of active disease (Figure 2A and 2B). On December 2021, patient underwent partial cystectomy with small bowel resection and anastomosis.

After that, the decision was to continue patient on adjuvant treatment, but patient refused.
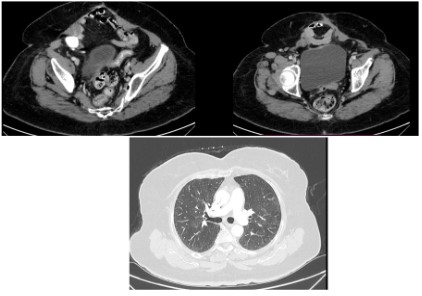
On February 2022, patient underwent whole body CT scan which shows new abdominal enhancing metastatic lesions in addition to new pulmonary nodules (Figure 3). Patient was diagnosed as a metastatic urachal adenocarcinoma.
So that decision was to start patient chemotherapy, which was Gemcitaben, 5FU, LCV. Cisplatin as protocol. Patient was complaining of chest infection and dyspnea with recurrent admissions to hospital with a complain of diarrhea and general fatigue as a complication of chemotherapy. Patient finished 4 cycles of Gem-FLP protocol with PET scan on May. 2022 showed stable disease. Due to intolerance of chemotherapy side effects.
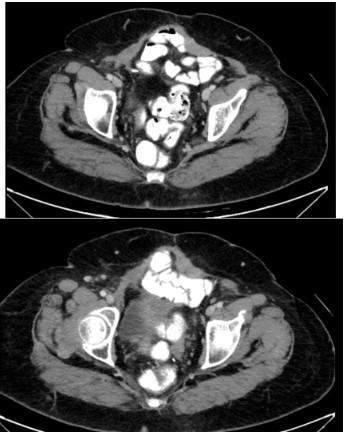
Genetic study was done and showed high MSI. So that, patient was started on Pembrolizumab as immunotherapy according to the results of genetic study. From August 2022 and until time of study writing, whole body CT scan studies show improvement in her condition with no evidence of active disease in her last study done on January 2023 (Figure 4). Her last PET scan also shows no evidence of active disease. Patient general condition dramatically improved with no any complain.
Hue and Jacquin first reported urachal tumours, which are uncommon and aggressive bladder tumours, in 1863. Only 0.5% of bladder cancers and 20% to 40% of primary bladder adenocarcinomas are attributable to them [7,2,13]. Less than 300 cases have been documented in the literature, and there have been no randomized studies to yet. As a result, there is a dearth of knowledge about the best ways to treat these tumors [4], specifically which chemotherapeutic drugs work best in atypical bladder cancers that share histological and biological characteristics with bowel cancers [10].
The urachus, a vestige of an embryonic structure that lies in the Retzius space between the transversalis fascia and the peritoneum on one side and the bladder dome and the umbilicus on the other, is the source of urachal malignancies [12,8]. Three layers make up the urachus: the outside layer is made of muscles, the middle layer is made of connective tissue, and the inner layer is often lined with transitional cell epithelium. The majority of urachal carcinomas are mucin-producing adenocarcinomas [5], which have an enteric type histology and signet ring cells more frequently found in colon malignancies [3,6]. Urachal malignancies can be diagnosed using the MD Anderson Cancer Center (MDACC) criteria [5,1,11].
These requirements include the presence of an enteric histology, a midline tumor location, a clear demarcation between the tumor and normal surface epithelium, the absence of urothelial dysplasia, cystitis cystica, or cystitis glandularis that transitions to the tumor, and the lack of a primary adenocarcinoma of another origin [9,11].All previous study no notice the genetic exam, the genetic exam is the golden core to treatment of the patient, Patient was diagnosed as a case of urachal adenocarcinoma with disease progression. So that decision was to start patient on new line of chemotherapy which was Gem-FLP protocol. Patient was complaining of chest infection and dyspnea with recurrent admissions to hospital with a complain of diarrhea and general fatigue as a complication of chemotherapy. Patient finished 4 cycles of Gem-FLP protocol with PET scan on May 2022 showed stable disease. Due to intolerance of chemotherapy side effects, genetic study was done and showed high MSI. So that, patient was started on Keytruda as immunotherapy according to the results of genetic study. From August 2022 and until time of study writing, whole body CT scan studies show improvement in her condition with no evidence of active disease in her last study done on January 2023 (Figure 4). Her last PET scan also shows no evidence of active disease. Patient general condition dramatically improved with no complain.