Introduction
Small round cell sarcomas are defined by malignant, round,
small, relatively undifferentiated cells. When a tumor is poorly
differentiated, identification of the diagnostic and morphological
features is difficult and therefore, no definitive diagnosis may be
possible [1]. Head and neck region are unusual sites for these tumors and obviously orbit is extremely rare [2]. Herein we present
an infant with an unusual huge hemorrhagic mass in his face that
invade inferior wall of right orbit.
Case presentation
During a routine fetal sonography of a pregnant woman at 37
weeks of gestational age radiologist reported a large echogenic
subcutaneous mass in right premaxillary region which didn’t exist
in previous sonography a week before. After delivery an infant
boy with pale appearance and a large hemorrhagic mass at right
face hiding the globe, was observed (Figure 1).
A blood test was done and hemoglobin was 13.1 and platelet
233000 at day one. On 3rd day sonography from brain and abdomen was unremarkable but a heterogeneous and hyperechoic
mass with a lot of vascularity and cystic spaces has revealed. As
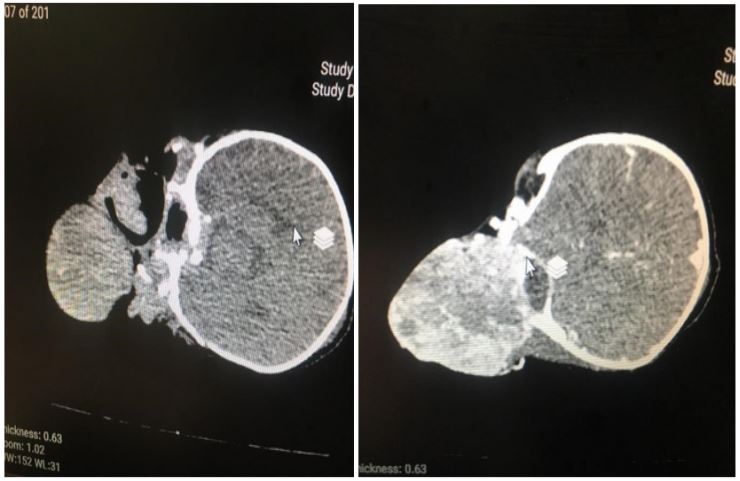
the infant was unstable, just a spiral CT scan with contrast could
be done that showed a huge exophytic lobulated enhanced mass
in right side of face and periorbita measuring 92 × 68 mm with hypervascularity and calcification. Bone destruction at right zygoma
and maxilla was noted too. The lesion extended into right orbit
and pushed globe superiorly (Figure 2).
Hemoglobin decreased to 8.3 due to necrosis and bleeding
from top of mass therefore FFP and packed cell injected and
condition stabilized. Because of bleeding property of mass and
the size of lesion which caused Kasabach-Merritt phenomenon.
The general condition got worse so tumor was resected wholly via
inferior transconjunctival orbitotomy approach and re-constriction was performed (Figure 3).
The infant was treated with chemotherapy. Lumbar punctate
was done for metastatic evaluation and result was negative. 7
days after first operation, a lateral tarsorrhaphy and debulking of
tumor performed. 4 months later the tumor relapsed at the same
site and biopsy revealed the same histopathology. Patient died
after 2 months.
Histopathological study
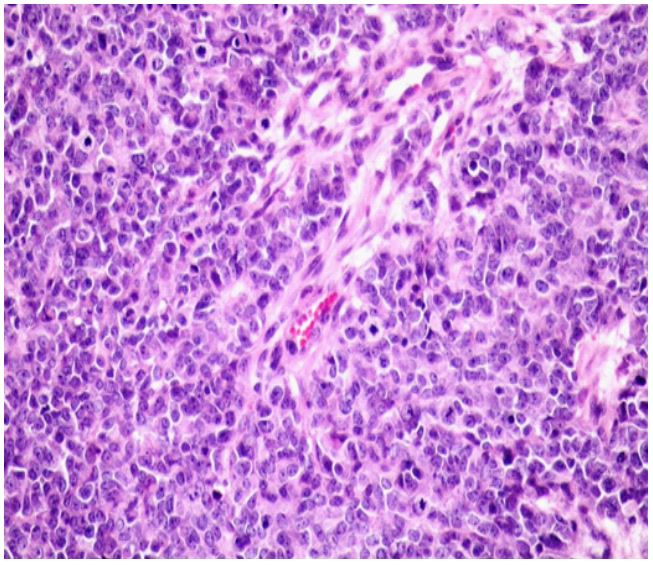
Round cell tumors are a group of highly invasive and malignant
tumors that can be divided into different types. This group is relatively small and uniform undifferentiated cells with increased nucleus to cytoplasm ratio [3]. Serial sections revealed diffuse sheets
of tumor cells with round oval nuclei vesicular chromatin arranged in rosette like formation in some areas. Necrosis, apoptosis
and nuclear debris are prominent (Figure 4).
In IHC staining, the mentioned cells showed positivity for CK,
EMA, CD99, vimentin, CD57 (few) and negative for LCA, NKX2,
chromogranin, synaptophysin, WT1, P40, PLAP and desmin. They
are in keeping with undifferentiated malignant small round cell
sarcoma.
Discussion
In Udifferentiated Small Round Cell Sarcomas (USRCS) prognosis is mainly poor [4]. They have an aggressive clinical course
with high rates of metastasis and lower sensitivity to chemotherapeutic protocols, with a 5-year survival of only 43% [5]. In 2020
the World Health Organization (WHO) classified soft tissue and
bone tumors and USRCS has four subgroups which include pleomorphic, spindle cell, round cell, and epithelioid subtypes [6]. Nowadays most cases of USRCS can be precisely categorize using a
combination of morphological, immunohistochemical, and molecular findings, however 10-20% cases cannot be classified into the
existing classifications [7] and needs more research [8]. So USRC
of orbit is extremely rare. There are seldom samples available to
guide treatment. Only 3 case reports have explained similar characteristics to this type of malignancy priorly and all were infants.
Mendelblatt et al. [9] reported a case of undifferentiated orbital sarcoma present at birth. The initial therapy consisted of exenteration and recurrence was treated by excision and radiation and
finally tumor proved fatal by cranial extension.
Gormley et al. [10] reported a congenital undifferentiated orbital sarcoma in a newborn with proptosis and a large right orbital mass. Despite treatment with chemotherapeutic regimen, the
tumor continued to grow, and she died at 11 weeks of age. Nowadays more advance immunohistochemical methods have been
developed and these methods determine tumor subtypes which
not used in these 2 studies.
3rd case is reported by Adesina et al. [11] which is a 6 month
old boy presented with recurrent, poorly differentiated orbital
sarcoma diagnosed as non-rhabdomyosarcoma soft tissue sarcoma, despite a subtotal resection of his orbital tumor and adjuvant
therapy with chemo-radio therapeutic regimen tumor recurrence
almost 2 years after initial diagnosis.
In these reports a combination of chemotherapy and radiotherapy is applied. As mentioned before due to the rarity of this type
of malignancy no specific treatment guidelines for USRCS are available. Main part of treatment is surgical resection with accurate
margin then accompanied with adjuvant radiotherapy and/or
chemotherapy [12]. Complete removal of tumor with 1 cm margin is the goal of surgery however in metastatic disease it can be
presumed as palliative treatment [13,14]. Biological risk factors
assigns the type of adjuvant therapy [15] but post or pre-operative radiotherapy are remarked as standard approaches [15] with
considering incongruity and rarity of this tumor, demonstrating
the efficacy of adjuvant chemotherapy is difficult so the advantage of this method is unsure and is not routinely recommended.
In our case due to the volume of mass and its bleeding property surgical debulking and primary repair at our center (Bahrami
eye center, tehran university of medical science, iran) has done
and for continuation of treatment a consult with pediatric oncology service applied and they recommended chemotherapy as post
operation adjuvant therapy. Unfortunately, seven times of different types of chemotherapy failed to save the patient. Despite the
advice of ophthalmologists to do radiotherapy, the parents and
the oncologist refused to let it to be done. But it could help us to
save the patient and we do not have enough information about
the chances because of the lack of studies on it.
Conclusion
In conclusion, we report a rare case of USRCS of the orbit, an
ultra-rare malignancy in this region, we made this diagnosis with
help of these characteristics: this tumor has small round cells with
hyperchromatic nucleus and hypo-chromatic cytoplasm, without
distinct differentiation, also immune histochemical findings were
positive for specific markers such as CD99. Aggressive multimodality therapy is needed however prognosis remains poor and
adjuvant radiotherapy and/or chemotherapy after wide surgical
excision is mandatory to improve prognosis.
References
- Sharma S, Kamala R, Nair D, Ragavendra TR, Mhatre S, et al. Round cell tumors: Classification and immunohistochemistry. Indian journal of medical and paediatric oncology: Official journal of Indian Society of Medical & Paediatric Oncology. 2017; 38: 349.
- Huang A, Patel N. Orbital desmoplastic small round cell tumor in an infant. Digital journal of ophthalmology: DJO. 2018; 24: 31.
- Gigantelli James W, Kincaid Marilyn C, Soparkar Charles NS, Lee Andrew G, Carter Susan R, et al. Orbital Solitary Fibrous Tumor: Radiographic and Histopathologic Correlations, Ophthalmic Plastic and Reconstructive Surgery: May 2001 - Volume 17 - Issue 3 - p 207-214.
- Watson S, Perrin V, Guillemot D, Reynaud S, Coindre JM, et al. Transcriptomic definition of molecular subgroups of small round cell sarcomas. The Journal of pathology. 2018; 245: 29-40.
- Bansal A, Goyal S, Goyal A, Jana M. WHO classification of soft tissue tumours 2020: An update and simplified approach for radiologists. European Journal of Radiology. 2021; 109937.
- Zhu J, Li B, Hu JJ, Liu W, Lu D, et al. Undifferentiated Small Round Cell Sarcoma of the Postcricoid Region of the Hypopharynx: A Rare Case Report and Review of the Literature. Onco Targets and therapy. 2021; 14: 4537.
- Choi JH, Ro JY. The 2020 WHO classification of tumors of soft tissue: selected changes and new entities. Advances in Anatomic Pathology. 2021; 28: 44-58.
- Sbaraglia M, Bellan E, Dei Tos AP. The 2020 WHO classification ofsoft tissue tumours: News and perspectives. Pathologica. 2020; 11: 1-15.
- Mendelblatt FI, Renpenning HJ. Congenital undifferentiated orbital sarcoma. Archives of Ophthalmology. 1964; 71: 459-462.
- Gormley PD, Thompson J, Aylward GW, Taylor D, Page AB. Congenital undifferentiated sarcoma of the orbit. Journal of pediatric ophthalmology and strabismus. 1994; 31: 59-61
- Ore-ofe OA, Zaugg BE, Dries DC, Palmer CA, Patel BC. Undifferentiated nonrhabdomyosarcoma soft tissue sarcoma of the orbit. Ophthalmic Plastic & Reconstructive Surgery. 2017; 33: e57-e60.
- Gómez J, Tsagozis P. Multidisciplinary treatment of soft tissue sarcomas: an update. World journal of clinical oncology. 2020; 11: 180.
- Dangoor A, Seddon B, Gerrand C, Grimer R, Whelan J, et al. UK guidelines for the management of soft tissue sarcomas. Clinical sarcoma research. 2016; 6: 1-26.
- Hall KS, Bruland ØS, Bjerkehagen B, Zaikova O, Engellau J, et al. Adjuvant chemotherapy and postoperative radiotherapy in highrisk soft tissue sarcoma patients defined by biological risk factors-A Scandinavian Sarcoma Group study (SSG XX). European Journal of Cancer. 2018; 99: 78-85.
- Gamboa AC, Gronchi A, Cardona K. Soft‐tissue sarcoma in adults: An update on the current state of histiotype‐specific management in an era of personalized medicine. CA: A cancer journal for clinicians. 2020; 70: 200-229.