Introduction
Bladder cancer (Bca) stands as one of the most prevalent malignancies affecting the human urinary system, with an estimated
430,000 new cases diagnosed annually [1]. In China, bladder cancer holds the top position among malignant tumors affecting the
urinary system, with 55,000 new cases per year, accounting for
1.8% of all tumors. The incidence rate is 3.0 per 100,000 population, representing 12.8% of all new cases worldwide [2]. Bladder cancer is three to four times more common in males than in females, and the peak age for diagnosis of Bca is between 60 and 70
years [1]. The incidence of Bca gradually increases with age. The
majority of fatal cases are attributed to muscle-invasive bladder
cancer (MIBC).
At present, the primary approach for treating MIBC is radical
cystectomy coupled with bilateral pelvic lymph node dissection.
In addition, a comprehensive treatment strategy incorporating drug-assisted chemotherapy is employed, either prior to, during,
or subsequent to the surgical procedure. Oxaliplatin, as a third-generation platinum-based anticancer drug, has a higher antitumor
activity and a lower toxicity compared to cisplatin. It is clinically
utilized alongside gemcitabine to treat advanced bladder cancer.
However, oxaliplatin still exhibits toxic side effects common to platinum drugs, particularly peripheral neurotoxicity, and there is a
significant heterogeneity among patients in terms of sensitivity to
chemotherapy and differences in toxic reactions. Hence, acquiring a more profound insight into the mechanism of oxaliplatin in
bladder cancer becomes imperative, allowing for dosage reduction while still achieving similar therapeutic effects.
Calcium ion (Ca2+) serves as the most ubiquitous second messenger, playing a vital role in intracellular signal transduction
and engaging in virtually all biological activities, encompassing
cellular proliferation and differentiation. In recent studies, multiple reports have substantiated the significant involvement of
calcium ions (Ca2+) in regulating cell apoptosis, but there is limited research on its impact on bladder tumors. The equilibrium
of intracellular calcium levels is upheld through the liberation of
Ca2+ from intracellular calcium reservoirs and the entry of extracellular calcium. The primary pathway for Ca2+ entry into tumor
cells is through Store-operated calcium entry (SOCE). SKF-96365
is a store-operated calcium entry inhibitor that significantly inhibits SOCE in non-excitable cells. The aim of this study is to clarify
and further comprehend the anticancer mechanism of oxaliplatin, particularly regarding calcium ions, which play a pivotal role
in cellular signal transduction. Exploring the role of inhibiting Ca2+
influx in inducing apoptosis in bladder cancer cells using a calcium
ion inhibitor is the main objective of this study. The results of the
study are reported as follows.
Methods
Cell culturing: Provided by Zhejiang University-Affiliated Sir
Run Run Shaw Hospital, the bladder cancer cell lines T24 and UMUC-3 were cultured in RPMI 1640 medium containing 10% (v/v)
fetal bovine serum (GIBCO, USA), 100 U/ml penicillin, and 50 μg/
ml streptomycin at 37°C in a 5% CO2
incubator.
Cell apoptosis test: Cell apoptosis was assessed using Annexin
V-FITC and flow cytometry. Bladder cancer cells were plated in a
6-well culture plate and exposed to RPMI 1640 medium containing 10 μM oxaliplatin (for calcium channel blockade experiments:
RPMI 1640 medium containing 10 μM SKF96365, 10 μM oxaliplatin, or 10 μM SKF96365+10 μM oxaliplatin), with a control group
included. After 24 hours of incubation, the cells were harvested,
rinsed with phosphate-buffered saline (PBS), fixed in 70% cold
ethanol, re-collected, and further washed with PBS to remove the
fixative. Subsequently, the cells were treated with RNAase overnight, followed by incubation with propidium iodide (PI) staining
solution. Flow cytometry was employed with an excitation wavelength of 488 nm to evaluate cell apoptosis and calculate the
apoptosis rate.
Measurement of Ca2+ concentration: Fluorescent calcium
probes and flow cytometry were used to measure intracellular
Ca2+ concentration in different cell groups. In a 6-well plate, bladder cancer cells were cultured at a density of 5×105
cells per well.
The cells were divided into different treatment groups, including
control group (without drug treatment) and groups treated with 10 μM oxaliplatin for 3,6,12, and 24 hours, respectively. The cells
underwent collection, two washes with PBS, trypsin-EDTA digestion, and were subsequently neutralized with culture medium
containing 10% FBS before being transferred into 1.5 ml EP tubes.
Following centrifugation at room temperature for 5 minutes at
2000 rpm, the supernatant was discarded, and the cells were
washed twice to ensure the removal of culture medium and residual trypsin. Fura-3A Staining: Fura-3A was diluted to 5 μM in
PBS. Except for well 1, which was re-suspended in PBS as a blank
control without adding dye, the remaining 6 wells were re-suspended with the diluted Fura-3A. Incubate at 37°C for 30 minutes.
Detection: After incubation, the samples underwent centrifugation at room temperature for 5 minutes, with a centrifugal speed
of 2000 rpm. Following this, the liquid portion (supernatant) was
removed, and the remaining solid components were dried using
absorbent paper. Subsequently, the samples were subjected to
two washes with PBS, followed by another round of drying using
absorbent paper. Finally, the samples were re-suspended in 1 ml
PBS and transferred to flow cytometry tubes for measurement.
Drugs and reagents: Oxaliplatin was manufactured by Jiangsu Hengrui Medicine Co., Ltd. (No: 06072117); Fluo-3A calcium
signaling fluorescent probe was supplied by Shanghai Biyuntian
Biotechnology Co., Ltd.; Annexin V-FITC kit was got from Shanghai
Biyuntian Biotechnology Co., Ltd.; SKF96365 was supplied by Sigma-Aldrich Corporation, USA.
Statistical methods: The statistical software used was SPSS
23.0. The mean ± standard deviation (x±s) was used to present
quantitative data. One-way analysis of variance (ANOVA) was employed for comparing multiple groups, and a significance level of
p<0.05 was applied.
Results
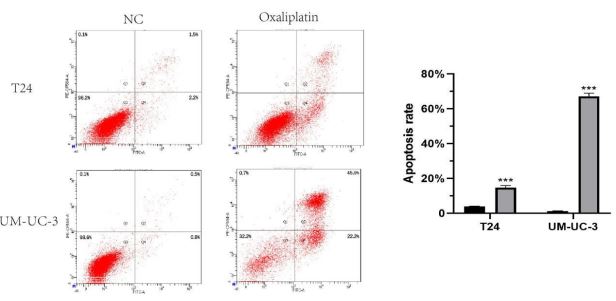
Apoptotic and growth-inhibitory effects of oxaliplatin on bladder cancer cells: According to previous literature, a concentration of 10 μM oxaliplatin for 24 hours was considered optimal
for oxaliplatin on bladder cancer cells. Apoptosis of cells in each
group was evaluated using flow cytometry analysis with the Annexin V-FITC apoptosis detection kit (Figure 1). Oxaliplatin treatment resulted in a significant increase in apoptosis among bladder cancer cells.
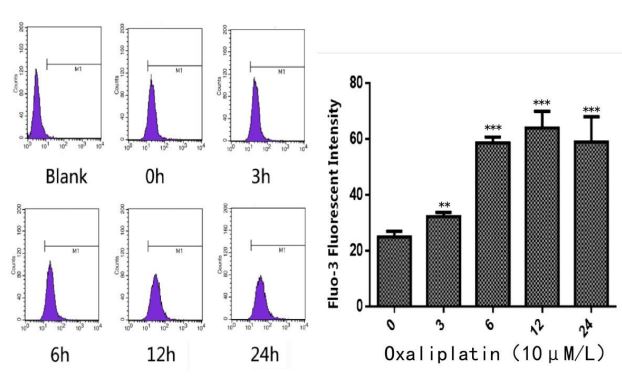
Intracellular Ca2+ concentration increasing significantly in T24
after oxaliplatin treatment: After treatment with oxaliplatin, most
tumor cells showed morphological changes, with enlarged round
shapes and irregular forms. Intracellular granules increased. From
Figure 2, The impact of oxaliplatin on ion levels within bladder
cancer cells was evident and significant. Oxaliplatin increased the
intracellular Ca2+ concentration, thereby affecting the apoptosis
of T24 cells.
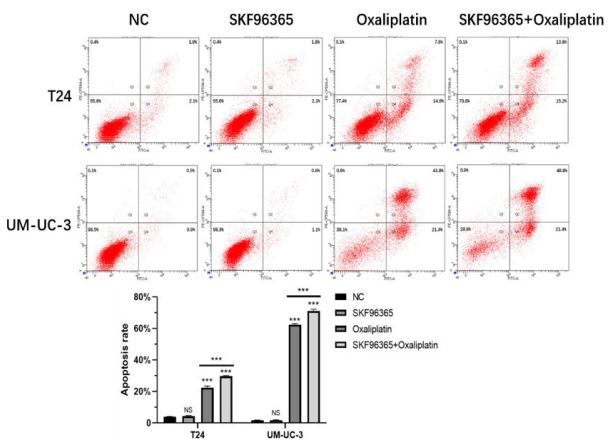
Blocking calcium ion enhances the apoptotic effect of oxaliplatin on bladder cancer cells: Next, we treated bladder cancer cells with RPMI 1640 medium containing 10 μM SKF96365,
10 μM oxaliplatin, 10 μM SKF96365+10 μM oxaliplatin respectively for 24 hours. The results from Figure 3 indicated that there
was no significant difference between the SKF96365 group and
the control group. However, both the oxaliplatin group and the
SKF96365+oxaliplatin group exhibited highly significant differences compared to the control group (p<0.001). Moreover, under the same conditions, the SKF96365+oxaliplatin group exhibited
significantly higher apoptosis compared to the oxaliplatin group
(p<0.001). This implies that the co-administration of SKF96365
and oxaliplatin exerts an increased apoptotic effect in cells affected by bladder cancer.
Discussion
Bladder cancer stands as the prevailing malignancy affecting
the urinary system, while the occurrence of this disease in China
has been on the rise in recent years, attributed to factors like smoking , environmental pollution and a long-term exposure to certain industrial chemicals. 70% of patients receive a diagnosis of
non-muscle-invasive bladder cancer (NMIBC), encompassing noninvasive papillary tumors (pTa), carcinoma in situ (CIS; pTis), and
early invasive tumors (pT1) [1]. Nevertheless, the recurrence rate
is notably high, ranging from 50% to 70%, and around 15% to 20%
of recurrent cases advance to muscle-invasive bladder cancer
(MIBC) or metastatic disease. Currently, the treatments for bladder cancer primarily involve surgery, with radiotherapy and chemotherapy preoperatively and postoperatively. MIBC can rapidly
progress and metastasize, resulting in a poor prognosis. Approximately 30% of newly diagnosed bladder cancer cases are already
MIBC. Radical cystectomy with pelvic lymph node dissection remains the established standard treatment for muscle-invasive
bladder cancer (MIBC), which can improve patient survival rates
and reduce risks of local recurrence as well as distant metastasis. However, tumor recurrence at distant sites frequently occurs
postoperatively, suggesting the presence of micro-metastases during surgery. Therefore, for cT2-cT4a MIBC patients, perioperative
chemotherapy is recommended to eradicate micro-metastases,
reduce tumor pathological staging, and minimize intraoperative
tumor implantation, thereby improving postoperative survival
rates.
Bladder urothelial carcinoma has shown sensitivity to platinum-based chemotherapy drugs. Oxaliplatin, a third-generation
platinum agent, is clinically effective for treating advanced bladder cancer and is often used alongside gemcitabine. Extensive
preclinical research has demonstrated that oxaliplatin is not crossresistant with cisplatin or carboplatin, and it has also exhibited
efficacy in cisplatin-resistant cell lines. Thus, oxaliplatin holds promise as an effective treatment for bladder cancer. Oxaliplatin has
demonstrated effectiveness in bladder cancer. International studies have confirmed the significant effects of postoperative oxaliplatin combined with gemcitabine or capecitabine in preventing
bladder cancer recurrence and treating advanced bladder cancer,
with relatively mild toxicity and side effects.
Research suggests that apoptosis could serve as a primary pathway through which oxaliplatin induces cell death in bladder cancer. Intracellular calcium (Ca2+) acts as a fundamental second messenger in cell signaling, exerting a pivotal function in regulating
cell proliferation, differentiation, and normal cellular activities [3].
Sustained elevation of intracellular calcium ion levels may be a
crucial cause of apoptosis. Under normal conditions, intracellular calcium signaling is maintained in a relatively balanced state
due to regulation by ion channels, ion pumps, and ion exchangers
[4,5]. Disruption of this balance may be associated with various
diseases such as cardiovascular diseases, immune deficiencies,
and malignancies. When cells are stimulated externally, it causes
changes in calcium ions, leading to apoptosis induced by the degradation of NO2
into oligomers [6,7].
Based on relevant reports, store-operated calcium entry
(SOCE) represents the principal calcium influx mechanism in nonexcitable cells, wherein calcium is released from intracellular stores. This process is primarily regulated by two proteins: STIM1
and Orai1 [8]. STIM1 acts as a calcium sensor on the endoplasmic
reticulum, while Orai1 is a calcium channel on the cell membrane.
When calcium is depleted from the endoplasmic reticulum, STIM1
dissociates from it and interacts with Orai1, leading to the opening
of Orai1 channels and the influx of extracellular calcium into the
cytoplasm. Recent studies have shown that in various malignant
tumors such as cervical cancer [9], liver cancer [10], lung cancer [11], renal cancer [12], and colorectal cancer [13,14], STIM1
and/or Orai1 are overexpressed. This abnormal SOCE signaling,
through various mechanisms promoting tumor growth, metastasis, and angiogenesis, contributes to the development of tumors
[15]. Therefore, we speculate that SOCE plays an important role in
oxaliplatin-induced apoptosis in bladder cancer.
In this experiment, we used fluorescent probe technology and
flow cytometry to observe the effects of oxaliplatin on bladder
tumor cells. The results showed that oxaliplatin significantly induced apoptosis in bladder cancer cells and increased intracellular calcium concentration. Based on the literature, we hypothesize that oxaliplatin may affect the permeability of bladder cancer
cell membrane calcium by translocating calcium across the membrane, leading to calcium influx and an increase in intracellular
free calcium concentration, which induces tumor cell apoptosis
and contributes to the killing of tumor cells. Therefore, we further
investigated the impact of the calcium antagonist SKF-96365 on
oxaliplatin-induced apoptosis in bladder tumor cells and found
that blocking calcium ions may enhance the apoptotic effect of
oxaliplatin.
Conclusion
Calcium could serve as a new target for Bca and calcium channel blocker combined with oxaliplatin can offer a new approach
for the therapy of bladder cancer.
References
- Patel VG, WK Oh, and MD Galsky. Treatment of muscle-invasive and advanced bladder cancer in 2020. CA Cancer J Clin. 2020; 70(5): 404-423.
- Jemal A, et al, Global cancer statistics. CA Cancer J Clin. 2011; 61(2): 69-90.
- Berridge MJ, P Lipp, and MD. Bootman. The versatility and universality of calcium signalling. Nat Rev Mol Cell Biol. 2000; 1(1): 11-21.
- Carafoli E. The calcium-signalling saga: tap water and protein crystals. Nat Rev Mol Cell Biol. 2003; 4(4): 326-32.
- Carafoli E. Calcium signaling: a tale for all seasons. Proc Natl Acad Sci U S A. 2002; 99(3): 1115-22.
- Rizzuto R, and T Pozzan. When calcium goes wrong: genetic alterations of a ubiquitous signaling route. Nat Genet. 2003; 34(2): 135-41.
- Parekh AB. Store-operated CRAC channels: function in health and disease. Nat Rev Drug Discov. 2010; 9(5): 399-410.
- Park CY, et al. STIM1 clusters and activates CRAC channels via direct binding of a cytosolic domain to Orai1. Cell. 2009; 136(5): 876-90.
- Chen YF, et al. Calcium store sensor stromal-interaction molecule 1-dependent signaling plays an important role in cervical cancer growth, migration, and angiogenesis. Proc Natl Acad Sci U S A. 2011; 108(37): 15225-30.
- Yang N, et al. Blockade of store-operated Ca(2+) entry inhibits hepatocarcinoma cell migration and invasion by regulating focal adhesion turnover. Cancer Lett. 2013; 330(2): 163-9.
- Li W, et al. The apoptosis of non-small cell lung cancer induced by cisplatin through modulation of STIM1. Exp Toxicol Pathol; 2013; 65(7-8): 1073-81.
- Kim JH, et al. Orai1 and STIM1 are critical for cell migration and proliferation of clear cell renal cell carcinoma. Biochem Biophys Res Commun. 2014; 448(1): 76-82.
- Wang JY, et al. STIM1 overexpression promotes colorectal cancer progression, cell motility and COX-2 expression. Oncogene. 2015; 34(33): 4358-67.
- Zhang Z, et al. STIM1, a direct target of microRNA-185, promotes tumor metastasis and is associated with poor prognosis in colorectal cancer. Oncogene. 2015; 34(37): 4808-20.
- Xie J, et al. SOCE and cancer: Recent progress and new perspectives. Int J Cancer. 2016; 138(9): 2067-77