Background
Sarcoidosis is a chronic systemic granulomatous disease of
unknown etiology. Breast involvement may occur in less than
1% of cases, often mimicking carcinomas at clinical examination,
making the differential diagnosis very challenging [1-3]. Only a
few cases with a primary presentation of this disease in the breast
tissue have been reported [3].
Case presentation
Female patient, 21 years old and with no comorbidities,
reports a palpable nodule associated with local pain and fever
that was noticed 2 months ago. Physical examination revealed
palpable bilateral axillary lymph nodes, a palpable nodule
occupying the lateral quadrants of the left breast and bullous skin
lesions, in addition to phlogistic signs in the same topography
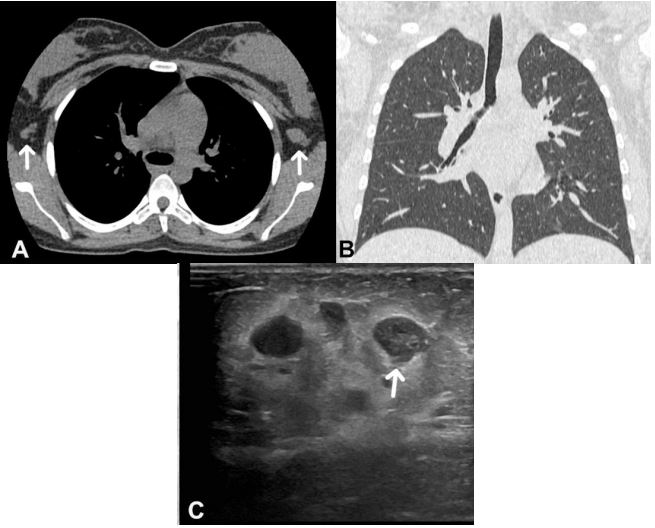
(Figure 1). Computed Tomography (CT) of the chest without
contrast was performed (Figures 2a and 2b), which only showed bilateral axillary lymph nodes enlargement. Ultrasonography of
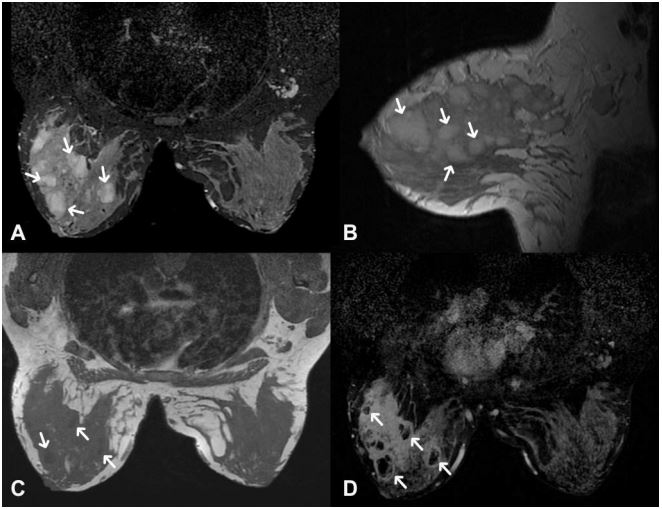
the breasts (Figure 2c) and Magnetic Resonance Imaging (MRI)
of the breasts with contrast revealed a solid-cystic complex in the
lateral quadrants of the left breast, in addition to bilateral axillary
lymph node enlargement, more evident on the left, which may
correspond to reactional process (Figures 3a-3d). Laboratory tests
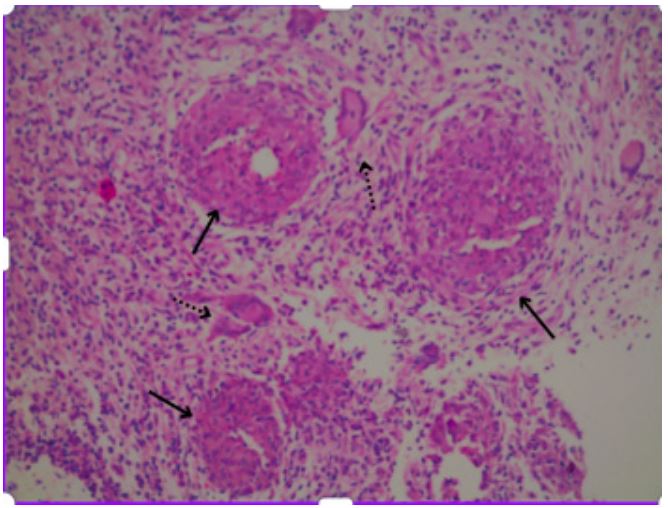
showed urinary calcium at the upper normal limit. Percutaneous
biopsy with histopathological result of breast fibroadipose tissue
showing numerous non-caseating granulomas with neutrophilic
microabscesses and Langerhans-type giant cells, suggesting
chronic granulomatous mastitis, which may correspond to
sarcoidosis (Figure 4). After treatment with corticosteroid therapy,
the lesions regressed.
Discussion
Sarcoidosis is a non-caseating granulomatous disease of
unknown etiology, predominantly in young to middle-age adults
(17-24 years old), which affects multiple tissues and organs,
including the lungs in most cases [1-3]. According to Ojeda et
al., there were only 35 cases of breast sarcoidosis between
1921 and 1997, in seven cases, a breast mass was the initial
manifestation of the disease [1]. In cases with breast tissue
involvement, there is usually a primary mediastinal focus,
which was not evident in this case. As no other primary focus is
identified, the infection is clinically called primary sarcoidosis of
the breast. On mammography, the mass can display well defined
contours or spicules, appearing as either a single mass or multiple
lesions. On ultrasound, a hypoechoic mass may show indistinct
borders that cannot be differentiated from malignancy. MRI findings may be similar of those seen in carcinoma of the breast,
including inhomogeneous signal intensity, irregular contours,
rapid enhancement and an early “washout” [1,3]. Diagnosis is
difficult due to multiple possible differential diagnoses, such as
inflammatory breast neoplasm, foreign body mastitis, diabetic
mastitis, tuberculous mastitis and other infectious diseases [1,2].
In view of such clinical findings as those found on this patient,
associated with these radiological images, despite its rarity,
primary breast sarcoidosis should be considered as a possible
diagnosis [4-6].
Conclusion
This case illustrates an unusual presentation of sarcoidosis
with breast involvement, which presents why primary sarcoidosis
should always be considered in case of isolated granulomatous
lesions despite its rarity. since malignancy must be excluded as a
primary differential diagnosis.
Declarations
Conflict of interest: The authors declare that they have no
conflict of interest.
Declarations: Consent for publication we obtained written
informed consent from the patient for publication.
Disclosures: None.
References
- Carvalho JF, Ramos CL, Ramos PM, de Sá Oliveira VF, de Araujo DB.
Sarcoidosis of the breast: an unusual clinical presentation. Revista
de Ciências Médicas e Biológicas. 2018; 17(3): 403-405. https://
doi.org/10.9771/cmbio.v17i3.23493
- Dutra AGA, Ferreira ACSDM, Araújo LDVCP, Tolentino FD, Bezerra
WF, et al. Sarcoidosis mimicking metastatic breast cancer-a case
report and literature review. Brazilian Journal of Oncology. 2023;
19: 1-7. https://doi.org/10.5935/2526-8732.20230354
- Endlich JL, Souza JA, Osório CABDT, Pinto CAL, Faria EP, Bitencourt
AGV. Breast sarcoidosis as the first manifestation of the disease.
The Breast Journal. 2019; 26(3): 543-544. https://doi.org/10.1111/
tbj.13560
- Rhazari M, Ramdani A, Gartini S, Bouali S, Aharmim M, et al.
Mammary sarcoidosis: A rare case report. Annals of Medicine
and Surgery. 2022; 78: 103892. https://doi.org/10.1016/j.
amsu.2022.103892
- Papanikolaou IC, Shigemitsu H. Sarcoidosis and breast cancer: A
retrospective case series. Respiratory Medicine Case Reports.
2020; 31: 101190.https://doi.org/10.1016/j.rmcr.2020.101190.
- Reis J, Boavida J, Bahrami N, Lyngra M, Geitung JT. Breast
sarcoidosis: Clinical features, imaging, and histological findings.
The breast journal. 2021; 27(1): 44-47. https://doi.org/10.1111/
tbj.14075.