Introduction
PCa is one of the most common malignant tumors in elderly
men. Approximately 30% of men are at risk of prostate cancer,
and the vast majority of patients have already developed distant
metastasis at the time of detection, with up to 66.3% developing
bone metastasis [1] and 3% of patients dying from mPCa [2].
Although the mortality rate is relatively low, symptoms such as
bone pain, spinal cord compression, pathological fractures and
other symptoms caused by bone metastases can greatly affect
patients’ quality of life.
Currently, Androgen Deprivation Therapy (ADT) is still the basic
treatment of mPCa. The main ADT methods include orchiectomy
or castration with administration of Gonadotropin Releasing
Hormone (GnRH) agonist, and the first-line use of ADT with
combined androgen blockade, such as with androgen receptor
antagonists (apalumide, enzalutamide, bicalutamide, etc. [3,4])
which is supported by several experiments. 90% of newly-treated
patients with mPCa may respond to ADT, but more than half of
patients with distant metastasis will develop hormone resistance
in less than 2 years and progress to metastatic castrationresistant prostate cancer. Thereafter, in addition to continuing
ADT, abiraterone, enzalutamide, Sipuleucel-T, and docetaxel can
be administered. For example, abiraterone inhibits androgen
synthesis by inhibiting CYP17, a key enzyme in androgen synthesis.
However, the median Overall Survival (OS) can only be extended
for about 4 months [5,6] with the use of abiraterone. Patients
will also be resistant to abiraterone, thus resulting in limited
clinical benefits. Although hormone therapy, targeted therapy,
immunotherapy or chemotherapy can be conducted if more
extensive bone metastases or even visceral metastases occur
after second-line treatment, the therapeutic effect is limited as
suggested in existing studies. For example, the median Progress
Free Survival (PFS) of chemotherapy as a subsequent treatment
after disease progression is only 3 months [7]. In addition, the
severe toxicity caused by chemotherapy can also affect the
metabolism and proliferation of normal cells, especially of some
elderly patients, which severely reduces their quality of life.
Eventually, chemotherapy resistance will develop, affecting the
subsequent treatment. According to guidelines of the National
Comprehensive Cancer Network (NCCN) for prostate cancer,
there are no effective drugs to treat this type of recurrent and
refractory castration-resistant prostate cancer.
In our recent clinical practice, a patient with mPCa who failed
treatments such as medical castration, and administration of
bicalutamide, abiraterone, and enzalutamide, developed multiple
new bone metastases throughout the body, pain in both legs and
even inability to walk, and his PSA continued to rise. Then TCM
treatment was conducted alone according to patient’s willingness.
The TCM treatment has achieved desired results. Bone related
pain was improved significantly in a short period of time, and the
corresponding serum PSA decreased rapidly. In the long-term
follow-up, the patient’s quality of life was greatly improved. Most
surprisingly, it was suggested from the patient’s recent bone scan
results that there were significantly fewer bone metastases than
before. This case is reported here. Permission was obtained, and
a written informed consent from the patient was presented in this
case.
Case report
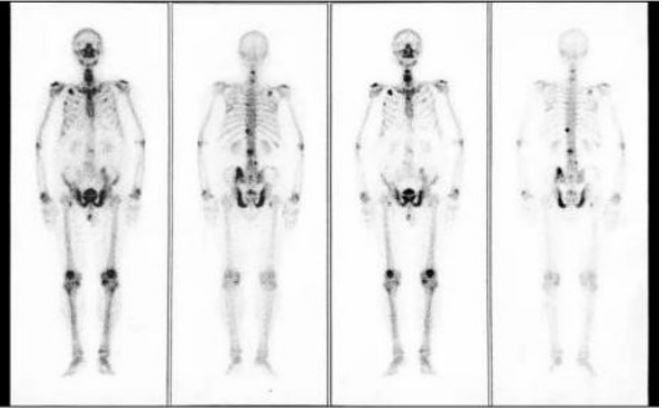
Liao, an 85-year-old male, presented with dysuria, pain in both
lower limbs with no obvious causes in July 2016, was diagnosed
with prostate cancer (T3, with a Gleason score of 5+3) by clinical
examination and prostate biopsy, with PSA>100 ng/ml at onset,
and bone scan suggesting signs of bone metastasis signs (Figure
1). After initiation of CAB with bicalutamide plus goserelin acetate
in August 2016, his PSA continued to decrease until June 2018.
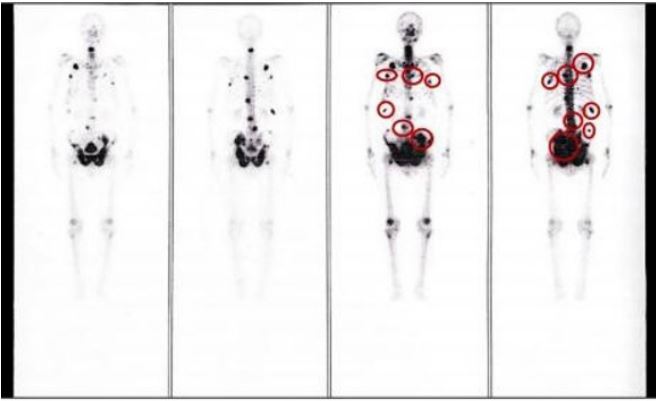
However, the patient experienced worsening bone related
pain, and multiplying PSA. There was no reliefin bone related
pain after sequential treatment with abiraterone acetate plus
prednisone, enzalutamide, and others. Patient’s PSA remained
high, and bone scan suggested new bone metastases in multiple
ribs, multiple segments of the spine and pelvis with signs of
extensive bone metastases (Figure 2). According to the NCCN
guidelines, there is no reliable treatment for prostate cancer,
and the patient expected to receive treatment with TCM. So, he
went to Affiliated Hospital of Chengdu University of TCM for TCM
treatment in July 2018. Before the initiation of TCM, the patient
was unable to move voluntarily due to bone pain, with serum PSA
of 128.91 ng/ml, NRS score of 7, and bone scan suggesting signs
of extensive bone metastases. Regarding the patient’s symptoms,
such as pain and discomfort, inability to walk, insomnia, and poor
appetite, he was diagnosed as impediment syndrome according
to TCM syndrome differentiation and treatment. Dangguiliuhuang
decoction was used as the main prescription with modification.
The main components were as follows: Radix angelicae sinensis
15 g, Rehmannia glutinosa 15 g, Stragalus membranaceus 60
g, Scutellaria baicalensis georgi 15 g, Coptidis rhizoma 6 g,
Phellodendron amurense 15 g, Radix rehmanniae preparata 15 g.
The administration was as follows: Put herbs above into the pot
for decocting. Then pour 2 liters of water. After the decoction is
boiled by the high fire, then turn to low fire and boil for about half
an hour. Each prescription is decocted twice and then mixed, and
is divided into two portions for administering for 2 days. Take it 3
times a day, 30-50 ml of it each time 1 hour after meal.
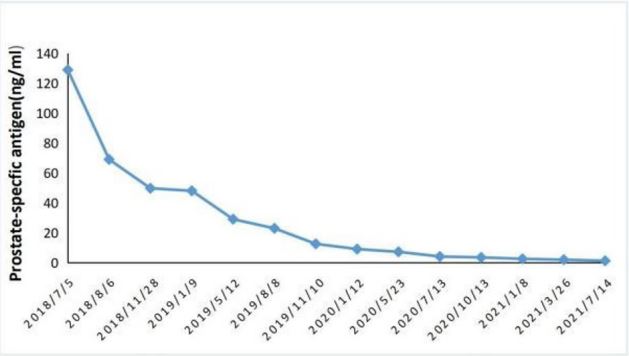
After undergoing TCM treatment for four weeks, the patient’s
pain, and symptoms such as fatigue, anorexia and insomnia were
remarkably relieved, and he could stand and walk briefly with the
help of tools, with a pain NRS score of 4, and his serum PSA was
reduced to 69 ng/ml. After 4 months of continuous medication,
the patient was able to walk on his own without relying on tools,
with a pain NRS score of 2, significant improvement in quality of
life, and a decrease in serum PSA to 79.7 ng/ml. In the subsequent
follow-up visits every three months, the patient’s general
symptoms and quality od life gradually improved, and the serum
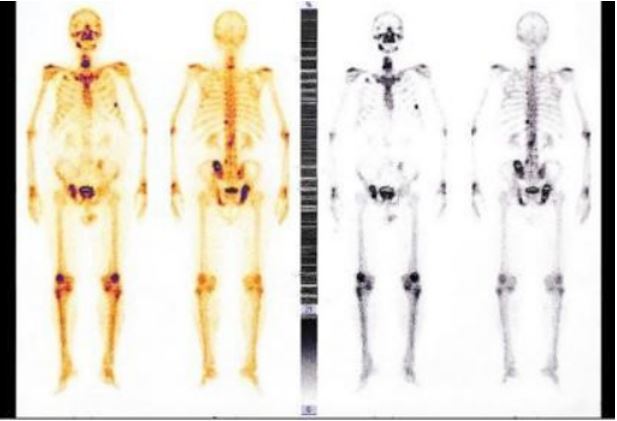
PSA also reduced (shown in Figure 4). The latest bone scan showed
a significant reduction in bone metastases (shown in Figure 3),
and no adverse events such as hepatic or renal impairment were
found during the follow-up.
Data availability statement: Data sharing is not applicable to
this article as no datasets were generated or analyzed 25 during
the current study.
Discussion
Prostate cancer is the second most common malignant tumor
in men. In China, the incidence rate of prostate cancer is increasing
year by year due to the aging of population and the changes in
diet [8]. Two thirds of patients have detected distant metastases
at the time of initial diagnosis [9], and the 5-year OSte cancer. It is
suggested by experts that the first-line use of ADT combined with
androgen patrate of mPCa is 30% [10]. At present, ADT remains as
the basic treatment of metastatic prostahway block, such as enzalutamide, can reduce the risk of death by 33% [11,12]. The oncological results of ADT achieved by surgical or medical castration
are similar. At present, medical castration has basically replaced
surgical castration [13], but long-term ADT treatment will lead to
hypogonadism, causing a series of adverse events such as osteoporosis, sexual dysfunction and cardiovascular disease, seriously
affecting the quality of life and even resulting in death [14,15].
More than 50% of patients with mPCa will develop metastatic
Castration-Resistant Prostate Cancer (mCRPC) within 2 years after
endocrine therapy, with a median OS of only 14 months [16].
The first-line treatment for patients with mCRPC is abiraterone,
enzalutamide, Sipuleuce lT, or docetaxel. Abiraterone is a CYP17
inhibitor. Although it has been reported that abiraterone can prolong the median OS and PFS of patients with mCRPC and delay the
time of pain progression [17], the effects are not ideal, especially
for patients who have received chemotherapy before. In a clinical
study of abiraterone acetate for mCRPC after chemotherapy, the
median OS of patients administered with abiraterone acetate plus
prednisone was only 14.8 months, and the median time to PSA
progression was only 5.6 months [18]. If the disease progresses
again, the clinical efficacy still remains limited although chemotherapy, immunotherapy, and targeted therapy, such as pembrolizumab, can be performed for subsequent treatment, the median
rPFS is only 3.7 months [19]. Therefore hormone resistance, chemotherapy resistance, disease progression and many other factors have driven us to find better treatment methods.
Fortunately, in this clinical practice, the patient with mPCa who
failed multiple lines of endocrine therapy chose TCM according to
his willingness. After treatment, the patient’s bone-related pain
improved significantly within a short period of time, and the corresponding serum PSA decreased rapidly, and the quality of life
improved greatly. It is especially worth noting that the latest bone
scans suggested a significant decrease in bone metastatic lesions.
And in the long-term follow-up, no adverse events occurred, and a very small economic cost was paid. Traditional Chinese medicine
has been used for thousands of years. The efficacy of TCM as an
adjuvant therapy in preoperative control of tumor progression,
postoperative recovery and prevention of recurrence [20], and
mitigation of toxicity and side effects during radiotherapy [21] has
been confirmed, but there are few reports on using TCM alone to
control tumors. TCM has been successfully practiced as a monotherapy to treat advanced Hepatocellular Carcinoma (HCC), which
has shown significant efficacy and high safety [22]. However, regarding TCM for treating recurrent and refractory castration-resistant prostate cancer, we reviewed relevant literatures on the
treatment of prostate cancer with TCM at home and abroad. We
found that all these treatments are based on single Chinese herbal medicine, Chinese herbal medicine extract, Chinese patent
medicine, acupuncture, patch and enema and other TCM treatment combined with endocrine therapy, chemotherapy or radiotherapy to treat prostate cancer, with the main purpose to reduce
the side effects of related treatments. This is the first case in the
world in which recurrent and refractory castration-resistant prostate cancer is treated with TCM alone.
The anti-tumor effect of traditional Chinese medicine has been
confirmed in many studies: 1) The direct anti-tumor effect of
TCM, such as Curcuma longa, Andrographis paniculata and other
Chinese herbal medicine extract can inhibit cell viability, induce
apoptosis and inhibit tumor growth [23,24]. 2) the role of TCM
in improving the tumor microenvironment. For example, studies
have shown that artemisinin derivatives [25], astragalus extracts
[26] can inhibit TGF-β in the tumor microenvironment because
the overexpression of Transforming Growth Factor-β (TGF-β can
lead to tumor microenvironment imbalance and tumor progression [27]. 3) TCM improving the body immunity. Studies have
reported that Panax ginsenghas a wide range of anti-cancer activity, because ginsenosides, the ginseng extract, can inhibit the
proliferation of tumor cells without affecting the vitality of normal
gastric epithelial cells. It shows anti-tumor effect while supporting
the healthy qi [28]. 4) the synergistic effect of the compound prescription. Each herb in the compound prescription has a variety of
anti-tumor active ingredients. And in the process of decoction,
every herb or several herbs can interact with and promote each
other. The mechanism of effect of TCM needs further research in
order to obtain greater benefits in clinical practice.
It is the first case in the world where TCM treatment alone has
achieved remarkable efficacy for the treatment of recurrent and
refractory castration-resistant prostate cancer, which provides a
new way for the treatment of it, as well as various treatments for
all stages of prostate cancer and other types of malignant tumors.
Abbreviations: MPCa: Metastatic Prostate Cancer; TCM: Traditional Chinese Medicine; PCa: Prostate Cancer; PSA: Prostate Specific Antigen; Pca: Prostate Cancer; ADT: Androgen Deprivation
Therapy; GNRH: Gonadotropin-Releasing Hormone; OS: Overall
Survival; PFS: Progress Free Survival; NCCN: National Comprehensive Cancer Network; MCRPC: Metastatic Castration-Resistant
Prostate Cancer; HCC: Hepatocellular Carcinoma; TGF-β: Transforming Growth Factor-β.
Declarations
Ethical approval: This study involving human participants was
reviewed and approved by the Medical Ethics Committee of the
Hospital of Chengdu University of Traditional Chinese Medicine
(No. 2015BL-003). And this study was performed in accordance
with the Declaration of Helsinki. The patient provided his written
informed consent to participate in this study.
Author contributions: Sq X: The patient was diagnosed and
treated in Traditional Chinese Medicine. Q Y, she contributed by
examining the patient, following up the patient, writing up the
manuscript, and reviewing the literature. J S, Jq Q, H M, P D, Ll
H, Dl W, all contributed by examining the patient, following up
the patient. Sq X guided writing and revised the manuscript. All
authors read and approved the final manuscript.
Conflict of interest statement: None of the authors have a
proprietary interest in this study or any conflicts of interest to disclose.
Funding: No funding was obtained for this study.
Competing interests: All authors declare no competing interests.
References
- Gandaglia G, Abdollah F, Schiffmann J, Trudeau V, Shariat SF, et al. Distribution of metastatic sites in patients with prostate cancer: A population-based analysis. Prostate. 2014; 74: 210-6.
- Awang ZH, Essler M, Ahmadzadehfar H. Radioligand therapy of metastatic castration-resistant prostate cancer: current approaches. Radiat Oncol. 2018; 13: 98.
- Kyriakopoulos CE, Chen YH, Carducci MA, Liu G, Jarrard DF, et al. Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer: Long-Term Survival Analysis of the Randomized Phase III E3805 CHAARTED Trial. J Clin Oncol. 2018; 36: 1080-7.
- Ingrosso G, Detti B, Scartoni D, Lancia A, Giacomelli I, et al. Current therapeutic options in metastatic castration-resistant prostate cancer. Semin Oncol. 2018; 45: 303-15.
- Rathkopf DE, Smith MR, de Bono JS, Logothetis CJ, Shore ND, et al. Updated interim efficacy analysis and long-term safety of abiraterone acetate in metastatic castration-resistant prostate cancer patients without prior chemotherapy (COU-AA-302). Eur Urol. 2014; 66: 815-23.
- Fizazi K, Scher HI, Molina A, Logothetis CJ, Chi KN et al. Abiraterone acetate for treatment of metastatic castration-resistant prostate cancer: Final overall survival analysis of the COU-AA-301 randomised, double-blind, placebo-controlled phase 3 study. Lancet Oncol. 2012; 248: 983-92.
- de Bono JS, Smith MR, Saad F, Rathkopf DE, Mulders PFA, et al. Subsequent Chemotherapy and Treatment Patterns After Abiraterone Acetate in Patients with Metastatic Castration-resistant Prostate Cancer: Post Hoc Analysis of COU-AA-302. Eur Urol. 2017; 71: 656-64.
- Chen W, Zheng R, Baade PD, Zhang S, Zeng H, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016; 66: 115-32.
- Chinese experts’ consensus on the treatment of metastatic prostate cancer 2018 256 edition]. Zhonghua Wai Ke Za Zhi. 2018; 56: 646-52.
- Zhang Z, Wei M, Mai L, Li Y, Wu J, et al. Survival Outcomes and Prognostic Analysis Following Greater Cytoreductive Radiotherapy in Patients with Metastatic Prostate Cancer. Front Oncol. 2020; 10: 549220.
- Sweeney CJ, Martin AJ, Stockler MR, Begbie S, Chi KN, et al. Overall Survival of Men with Metachronous Metastatic Hormone-sensitive Prostate Cancer Treated with Enzalutamide and Androgen Deprivation Therapy. Eur Urol. 2021; 80: 275-9.
- Davis ID, Martin AJ, Stockler MR, Begbie S, Chi KN, et al. Enzalutamide with Standard First-Line Therapy in Metastatic Prostate Cancer. N Engl J Med. 2019; 381: 121-31.
- Tan YG, Poon RJ, Pang LJ, Villanueva A, Huang HH, et al. Comparative study of surgical orchidectomy and medical castration in treatment efficacy, adverse effects and cost based on a large prospective metastatic prostate cancer registry. Urol Oncol. 2020; 38: 682.e1-e9.
- Kintzel PE, Chase SL, Schultz LM, O’Rourke TJ. Increased risk of metabolic syndrome, diabetes mellitus, and cardiovascular disease in men receiving androgen deprivation therapy for prostate cancer. Pharmacotherapy. 2008; 28: 1511-22.
- Braga-Basaria M, Dobs AS, Muller DC, Carducci MA, John M, et al. Metabolic syndrome in men with prostate cancer undergoing long-term androgen-deprivation therapy. J Clin Oncol. 2006; 24: 3979-83.
- Kirby M, Hirst C, Crawford ED. Characterising the castration-resistant prostate cancer population: a systematic review. Int J Clin Pract 2011; 65: 1180-92.
- Basch E, Autio K, Ryan CJ, Mulders P, Shore N, et al. Abiraterone acetate plus prednisone versus prednisone alone in chemotherapy-naive men with metastatic castratio resistant prostate cancer: Patient-reported outcome results of a randomised phase 3 trial. Lancet Oncol. 2013; 14: 1193-9.
- de Bono JS, Logothetis CJ, Molina A, Fizazi K, North S, et al. Abiraterone and increased survival in metastatic prostate cancer. N Engl J Med. 2011; 364: 1995-2005.
- Antonarakis ES, Piulats JM, Gross-Goupil M, Goh J, Ojamaa K, et al. Pembrolizumab for Treatment-Refractory Metastatic Castration-Resistant Prostate Cancer: Multicohort, Open Label Phase II KEYNOTE-199 Study. J Clin Oncol. 2020; 38: 395-405.
- Zhang W, Zhang B, Chen XP. Adjuvant treatment strategy after curative resection for hepatocellular carcinoma. Front Med. 2021; 15: 155-69.
- Yang J, Zhu L, Wu Z, Wang Y. Chinese herbal medicines for induction of remission in advanced or late gastric cancer. Cochrane Database Syst Rev. 2013: Cd005096.
- Wang L, Ke J, Wang C, Li Y, Wu G, et al. Efficacy and Safety of Banxia XieXin Decoction, a Blended Traditional Chinese Medicine, as Monotherapy for Patients with Advanced Hepatocellular Carcinoma. Integr Cancer Ther. 2020; 19: 1534735420942587.
- Chun JY, Tummala R, Nadiminty N, Lou W, Liu C, et al. Andrographolide, an herbalmedicine, inhibits interleukin-6 expression and suppresses prostate cancer cell growth. Genes Cancer. 2010; 1: 868-76.
- Zhai B, Zhang N, Han X, Li Q, Zhang M, et al. Molecular targets of β-elemene, a 297 herbal extract used in traditional Chinese medicine, and its potential role in cancer therapy: A review. Biomed Pharmacother. 2019; 114: 108812.
- Yao Y, Guo Q, Cao Y, Qiu Y, Tan R, et al. Artemisinin derivatives inactivate cancer-associated fibroblasts through suppressing TGF-β signaling in breast cancer. J Exp Clin Cancer Res. 2018; 37: 282.
- Wei Y, Wu Y, Feng K, Zhao Y, Tao R, et al. Astragaloside IV inhibits cardiac fibrosis via miR-135a-TRPM7-TGF-β/Smads pathway. J Ethnopharmacol. 2020; 249: 112404.
- Wade CA, Kyprianou N. Profiling Prostate Cancer Therapeutic Resistance. Int J Mol Sci 2018; 19.
- Wang X, Su GY, Zhao C, Qu FZ, Wang P, et al. Anticancer activity and potential mechanisms of 1C, a ginseng saponin derivative, on prostate cancer cells. J Ginseng Res. 2018; 42: 133-43.