Introduction
The adverse effects of chemotherapy on the Central Nervous
System (CNS) are widely known; These can manifest under a variety of neurological syndromes such as acute, subacute, chronic
encephalopathies, cerebellar dysfunction, cognitive dysfunction,
reversible posterior encephalopathy, myelopathies or even meningitis [1]. Certain chemotherapy drugs are often associated with
neurotoxicity such as Ifosfamide, Methotrexate, but also 5-Fluorouracil (5-FU), especially in high doses [2].
Capecitabine is a precursor of 5-FU, which it quickly replaced
in the last 20 years, especially in the treatment of gastrointestinal
or breast cancers, due to the oral route of administration, considered easier for elderly oncology patients [3].
Capecitabine, a fluoropyrimidine carbamate, was designed
with the exact aim of delivering 5-FU selectively to tumor cells,
being initially metabolized in the liver and later, in the final stages
of transformation, in the tumor cells. This compound is initially
absorbed intact, being then metabolized into the final product in
the form of 5-FU with cytostatic action in three stages; As a first step, under the action of hepatic carboxylesterase, capecitabine
is transformed into 5’-deoxy-5-fluorocytidine, which will later
become 5’-deoxy-5-fluorouridine under the influence of cytidine
deaminase found in the liver and in tumor cells. In the third stage,
5’-deoxy-5-fluorouridine is converted into 5-FU with the help of
thymidine phosphorylase, the enzyme whose activity has been
shown to be significantly higher in tumor formations than in healthy body tissues. Thus, due to the fact that this metabolic chain
occurs mainly in tumor tissue, capecitabine has the advantage of
minimal toxic exposure of healthy tissue with maximum targeting
of the active substance to the targeted pathological formation
[4,5].
Encephalopathy caused by 5-FU is often mentioned in medical
literature, however, in the case of Capecitabine, only a few cases
of neurotoxicity have been documented; In most cases found, the
symptoms disappeared shortly after stopping the medication,
with the help of conservative treatment. Variants of mutations in
Dihydropyrimidine Dehydrogenase (DPD), a liver enzyme that facilitates the elimination of 5-FU metabolites, may explain the toxic
effects of Capecitabine. Although the relationship between DPD
deficiency and Capecitabine neurotoxicity could not be confirmed
in all cases, enzyme testing is recommended to be done, especially in the case of elderly patients [6,7].
Case report
The 82-year-old patient, diagnosed with stage pT3pN0Mx sigmoid colon adenocarcinoma, for which she underwent a surgical
intervention approximately two months ago, currently being treated at home with Capecitabine 4 g/day, is brought to the emergency room by her family for an episode of confusion. This symptomatology started approximately 12 hours before presentation,
when the patient called her relatives in the middle of the night to
have a simple conversation; Following that, in the morning of the
same day, her niece found her wearing sunglasses at home and
trying to talk on the phone holding the device to the nose. The
relatives state that this episode occurred suddenly, in apparent
good health, the patient having a normal behavior the day before
the presentation to the emergency room. From the patient’s history, we note that she was diagnosed 4 years ago with a malignant
jejunal tumor, for which she was treated with Capecitabine. Neurological examination performed at the time of presentation reveals a confused patient, with difficult cooperation, disorientated
temporospatially, who partially executes simple commands, does
not execute complex commands, does not respond adequately to
questions, with echolalia but without motor deficit and with symmetrically deep tendon reflexes.
Routine blood tests performed at the emergency department
showed a mild lymphopenia with no signs of infection, myelosuppression, electrolytic disturbance, renal or hepatic impairment.
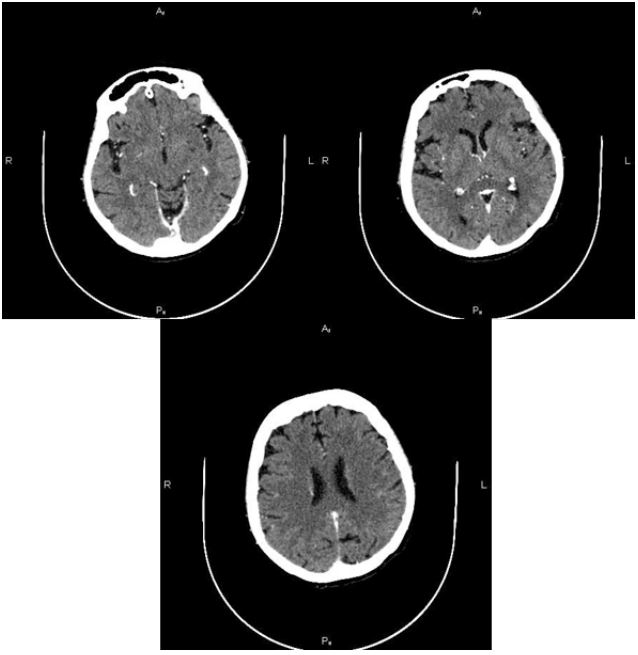
Cerebral computed tomography performed, without and with
contrast, does not reveal pathological tomodenstiometric lesions
of an acute nature, nor pathological intakes of the gadolinium
substance. The patient remains under observation in the neurology department, and in the following hours, after stopping the chemotherapy treatment and under intense hydration, the patient’s
condition improves rapidly, with the remission of the confusional
syndrome and the language disorder in less than 24 hours.
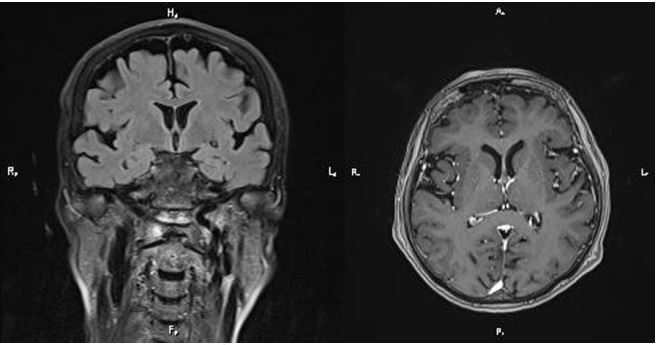
Thus, after 48 hours from the onset of the symptoms, a brain
MRI was performed, which did not reveal signal abnormalities,
but only a few demyelinating lesions at the level of the bilateral
frontal lobes, with a microangiopathic substrate and no enhancement upon gadolinium administration was observed.
With the high suspicion of a toxic effect of capecitabine, the
patient was tested for the most prominent mutations of the DPD
gene (variant DPYD E412E (HapB3), variant DPYD I560S (*13), variant DPYD IVS14+1G>A (*2A), variant DPYD D949V) who came
out negative a few days later. The attending oncologist is contacted and it is decided, with the patient’s consent, to stop treatment
with Capecitabine.
The patient was reevaluated one month later without any pathological changes being detected during the neurological examination. She is still under oncological supervision and no other line
of chemotherapy was prescribed in her case.
Discussion
Capecitabine is an oral chemotherapy, which is becoming more
and more popular these days, being preferred instead of its precursor, 5-FU, due to the easy way of administration [8].
The encephalopathy caused by 5-FU has many ways of presentation such as states of confusion, behavior disorders or seizures,
the diagnosis being based on the following criteria [9]:
- Appearance of signs and symptoms during treatment or
shortly after completion of treatment.
- Exclusion of other causes that could explain the patient’s
symptoms, such as hypo- or hyperglycemia, altered serum
electrolyte levels, liver failure, sepsis, azotemia or CNS neoplasms.
- Exclusion of adverse effects determined by concomitantly
administered medication.
Despite its widespread use in medical practice, little information is known about the toxicity of Capecitabine on the CNS, being
only a few cases published in the literature. Cases of induced CNS
toxicity manifested by memory disorders, episodes of confusion,
psychiatric disturbances, ataxia, speech disorder such as dysarthria, or even seizures have been described [10,11].
We present a case of reversible toxic encephalopathy, due to
treatment with capecitabine, which appeared on the eighth day
of administration, being the second cycle of treatment with this
chemotherapy in the patient’s life. Published material report latency period until the installation of the clinical picture which varies between 3 days to 3 months after the initiation of this treatment [9].
Brain imaging, especially brain MRI, varies from none to
changes in the white matter, most of the time in both cerebral
hemispheres [6,9]. In the present case, brain imaging did not
identify pathological changes that could be correlated with the
patient’s symptoms, but the investigation was carried out more
than 48 hours after the onset of the symptoms and after stopping
the treatment.
Regarding the etiopathogenic mechanism, several hypotheses
have been launched that must be analyzed. Starting from the
known fact that 5-FU toxicity is significantly higher among the
female population, Manuela Fantini et al, in a literature review
published in 2010 [6], she launches the hypothesis according to
which toxicity could be caused by DPD deficiency. Although the
relationship with enzyme deficiency could not be demonstrated
in all patients, its dosage is still recommended, especially in elderly patients. Testing for mutation of the DPD gene came out
negative in the case of our patient. In addition, it is known that
Capecitabine can penetrate the BBB, thus reaching the level of
the CNS, where it can be metabolized into 5-FU, then manifesting
its toxic effects at this level. Thus, the toxic effect of the substance
on the vascular endothelium with the temporary alteration of the
protective barrier of the nervous system must also be taken into
account [9].
These being presented, whenever there is an alteration of
the neurological status during treatment with Capecitabine, reversible toxic encephalopathy should be considered, especially in the case of elderly patients. The patients’ clinic and imaging
findings differ from one patient to another, the evolution being
favorable, with the remission of symptoms shortly after stopping
the treatment. Although it is a rare adverse reaction, it should
not be neglected as additional tests are required. Thus, once this
pathology is suspected, it is recommended to immediately stop
the treatment with the application of the necessary supportive
treatments, after excluding other causes that could explain the
symptoms [12].
Capecitabine remains a preferred chemotherapeutic in current
practice, but adverse neurological effects must be carefully monitored, especially for the population at risk.
References
- Taillibert S, Le Rhun E, Chamberlain MC. Chemotherapy-Related Neurotoxicity. Curr Neurol Neurosci Rep. 2016; 16(9). http: //dx.doi.org/10.1007/s11910-016-0686-x
- Chue AL, Fernando IN, Hussain SA, Yates DA. Chemotherapy related encephalopathy in a patient with stage IV cervical carcinoma treated with cisplatin and 5-fluorouracil: A case report. Cases J. 2009; 2(7): 1-5.
- Endo A, Yoshida Y, Nakashima R. A Case Report and Review of the Literature. 2013; 417-20.
- Hoff PM, Ansari R, Batist G, Cox J, Kocha W, et al. Comparison of oral capecitabine versus intravenous fluorouracil plus leucovorin as first-line treatment in 605 patients with metastatic colorectal cancer: Results of a randomized phase III study. J Clin Oncol. 2001; 19(8): 2282-92.
- Alqahtani S, Alzaidi R, Alsultan A, Asiri A, Asiri Y, et al. Clinical pharmacokinetics of capecitabine and its metabolites in colorectal cancer patients. Saudi Pharm J. 2022; 30(5): 527-31.
- Fantini M, Gianni L, Tassinari D, Nicoletti S, Possenti C, et al. Toxic encephalopathy in elderly patients during treatment with capecitabine: Literature review and a case report. J Oncol Pharm Pract. 2011; 17(3): 288-91.
- Martens FK, Huntjens DW, Rigter T, Bartels M, Bet PM. DPD Testing Before Treatment With Fluoropyrimidines in the Amsterdam UMCs : An Evaluation of Current Pharmacogenetic Practice. 2020; 10: 1-10.
- Comella P. A review of the role of capecitabine in the treatment of colorectal cancer. 2007; 3(3): 421-31.
- Lyros E, Walter S, Keller I, Papanagiotou P, Fassbender K. Subacute reversible toxic encephalopathy related to treatment with capecitabine: A case report with literature review and discussion of pathophysiology. Neurotoxicology. 2014; 42: 8-11. Available from: http: //dx.doi.org/10.1016/j.neuro.2014.02.010
- Marrone LCP, Marrone BF, Gadonski G, Marrone ACH, da Costa JC. Posterior reversible encephalopathy syndrome. Clin Adv Hematol Oncol. 2012; 10(9): 614-5.
- Padhi P. Current Problems in Cancer: Case Reports Acute mania due to capecitabine and oxaliplatin in a patient with metastatic colorectal cancer. Curr Probl Cancer Case Reports. 2023; 9: 100225. https: //doi.org/10.1016/j.cpccr.2023.100225
- Monti M, Barone D, Amadori E, Bartolini G, Ruscelli S, et al. Posterior reversible encephalopathy syndrome: A rare neurotoxicity after capecitabine. J Oncol Pharm Pract. 2020; 26(7): 1795-801.