Introduction
Choriocarcinoma is a germ cell tumor containing syncytiotrophoblastic cells that secrete β-Human Chorionic Gonadotropin (β-HCG). While choriocarcinoma originating in the gonads frequently metastasizes to the lungs, Primary Pulmonary Choriocarcinoma (PPC) originating in the lungs is extremely rare, particularly in males. A review of the literature revealed only 41 reported cases of male PPC. SMARCA4 (BRG1) is one of the catalytic subunits of the SWI/SNF complex, crucial for chromatin remodeling. Mutations or deletions in the SWI/SNF complex subunits can lead to tumorigenesis. Recent studies have shown that SMARCA4 deficiency is associated with highly malignant undifferentiated tumors, especially those in the thoracic cavity, though these cases are rare. Additionally, SMARCA4 expression loss is found in about 5.1% of Non-Small Cell Lung Cancer (NSCLC) cases. However, no previous reports have described male primary pulmonary choriocarcinoma with concurrent SMARCA4 loss.
Case presentation
The patient, a 54-year-old male, was found to have occupied left lung for 2 days by physical examination, and had no discomfort such as fever, cough, or chest pain, and no prior history of tumor. She was admitted to our hospital on March 28, 2023 for further treatment. Chest CT showed space occupying the upper lobe of the left lung and the hilar of the left lung, multiple enlargement of mediastinal lymph nodes, multiple nodules in both lungs, local pleural thickening on the left side and dense soft tissue nodules (Figure 1). A single aperture thoracoscopic excision of the upper lobe of the left lung was performed, and the excised tissue was sent for pathological examination.
Pathological findings
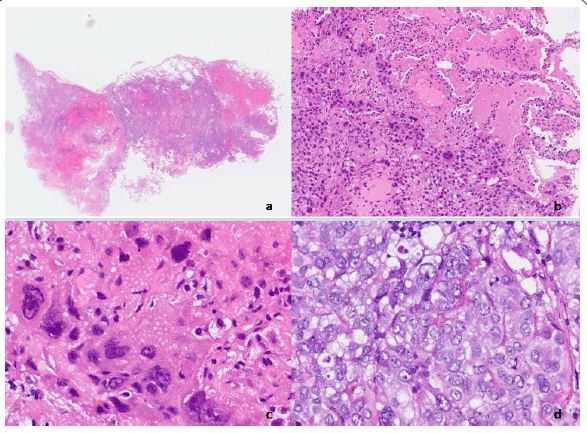
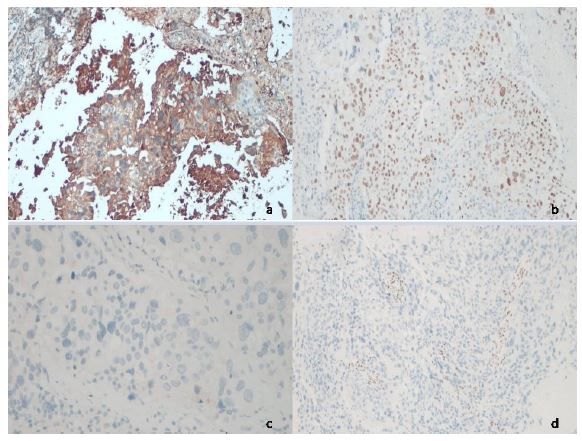
Pathological examination: There was 1 wedge-shaped excised lung tissue specimen with anastomotic nails, the size of which was 9.0 cm x 6.0 cm x 2.5 cm. A large hemorrhage necrotic lesion was found adjacent to the anastomotic nail’s broken end, the range being 5.0 cm x 4.5 cm x 3.0 cm. The lesion is soft in texture, gray-red and/or dark-red in section, and invades the visceral pleura. Under the mirror (Figure 2): Tumor tissue grows invasively along the alveolar wall in the lung parenchyma, with extensive bleeding and necrosis. Tumor cells have two main forms, one is large and heterotypic syncytiotrophoblastic cells, and the other is medium sized round and/or epithelioid cells arranged in sheets, with abundant cytoplasm, pale eosinophilic or clear. The chromatin is fine or vacuolar, the nucleolus is obvious, and the mitotic image is easy to see and >5/10HPF. Immunohistochemical staining of tumor cells showed (Figure 3): Human Chorionic Gonadotropin (HCG), broad-spectrum Cytokeratin (CKpan), CD10 and SALL4 were all positive, while cytokeratin (CK7) and GATA3 were slightly positive. NapsianA, P40, P63, OCT3/4, Chromaffin A (CgA), Syn, CD56, vimentin, CD34, CD117 and Thyroid Transcription Factor (TTF1) were negative, and SMARCA4 (BRG1) protein expression was missing, INI1 (SMARCB1) protein expression, Ki-67 positive index hot spot about 60%.
Pathological diagnosis
“Left lung” highly malignant tumor with excessive bleeding and necrosis, combined with clinical, immunohistochemical and blood HCG indicators, consistent with primary choriocarcinoma of the lung with SMARCA4 deletion.
Note: This is a rare tumor in male patients and tends to differentiate from somatic cell derived tumors (lung non-small cell carcinoma) into choriocarcinoma. Such tumour is different from female germ cell sources associated with pregnancy velvet carcinoma. Regular monitoring of blood HCG is recommended. After surgery (April 21, 2023), blood HCG>10000 mIU/ml was detected.
Treatment and follow-up
The patient underwent left upper lobectomy and received 8 cycles of chemotherapy (etoposide + cisplatin, 6 cycles; Bleomycin + etoposide + cisplatin, 2 cycles). The patient’s blood HCG level was regularly monitored after surgery and remained at a high level for a long period of time, with the last check of blood β-HCG reaching 14062.00 mIU/mL about 8 months after surgery (November 24, 2023). When followed up to 7 months after the operation, the patient had multiple systemic metastases in liver, kidney, bone, thyroid, etc. The survival with this kind of tumor is generally poor and now the patient has been dead.
Discussion
Choriocarcinoma is a germ cell tumor containing syncytiotrophoblast cells and secreting β-Human Chorionic Gonadotropin (β-HCG). Choriocarcinoma of pregnancy originating in the gonads often metastasizes to the lungs, but Primary Pulmonary Choriocarcinoma (PPC) originating in the lungs is very rare [1], especially in men [2]. SMARCA4 (BRG1) is one of the two catalytic subunits of the yeast switch/sucrose non-fementable complex (SWI/SNF) complex. SWI/SNF complex consists of three subunits: ATPase catalytic subunit SMARCA4 (BRG1) /SMARCA2 (BRM); Highly conservative core subunits INI1 (SMARCB1, SNF5, and BAF47), SMARCC1 (BAF155), and SMARCC2 (BAF170); And functional specific helper subunits PBRM1 (BAF180) and ARID1A (BAF250A). Deletion or mutation of the catalytic subunits and core subunits of SWI/SNF complex in the somatic or embryonic background can result in inactivation of coding proteins and abnormal overall function of the complex, leading to tumorigenesis [3]. Recent reports have shown that SMARCA4 deletion can be seen in some highly malignant undifferentiated tumors, especially SmarCA4-DUT in the thoracic cavity, which has received more attention, but it is very rare. So far, less than 100 cases of SmarCA4-DUT have been reported [4]. In addition, SMARCA4 expression loss is also found in about 5.1% of Non-Small Cell Lung Cancer (NSCLC) [5]. However, PumbMed has not found any case reports of male primary pulmonary choriocarcinoma accompanied by SMARCA4 loss.
Primary Pulmonary Choriocarcinoma (PPC) is a rare and highly malignant tumor. These patients lack specific clinical features, but there are also literature reports that patients may have symptoms such as cough, chest pain, dyspnea or superior vena cava syndrome [6]. The patient in this case is an elderly male who has been in good health in the past, without any discomfort, and the blood β-HCG level has not been detected before surgery, which makes it difficult to diagnose primary pulmonary choriocarcinoma in a timely and early stage, and may even be missed or misdiagnosed. The microscopic morphology of choriocarcinoma showed that the tumor cells were nested and solid, with extensive bleeding and necrosis. It consists of mononuclear trophoblastic cells (including cytotrophoblastic cells and intermediate trophoblastic cells) and large multinucleated giant cells (syncytiotrophoblastic cells).
Syncytiotrophoblastic cells exhibit characteristic HCG immunomarker positive cytoplasm. Immunohistochemistry plays an important role in the diagnosis of PPC. Studies have suggested that positive GATA-3, CK7, p63, p40, CD10, and negative CK5/6, TTF-1, Napsin A are important tips for the diagnosis of choriocarcinoma [7]. It has also been suggested that the expression of GATA-3 may be a tissue-specific marker of trophoblast differentiation, which is of great significance for the diagnosis of choriocarcinoma [8]. It has also been reported that CK7, AE1/AE3 and CD10 may be positive in pulmonary choriocarcinoma, while TTF-1 may be negative [9]. In this case, first of all, the lesions were characterized by exextensive bleeding and necrosis, which was one of the clues for the diagnosis of choriocarcinoma. In addition, microscopically, tumor cells can be observed in two main forms: one is large and heterotypic syncytiotrophoblastic cells with characteristic HCG expression; the other is rounded and/or epithelioid cells with nest and lamellar arrangement, fine vacuolar nuclear chromatin, distinct nucleoli, and easy to see mitotic images (>5/10HPF), and abundant cytoplasm. Pale eosinophilous or vacuous. SMARCA4 was deexpressed in all tumor cells, and CK, GATA3, SALL4, CD10 expression was positive, while TTF-1 expression was negative, which was consistent with the immunohistochemical results reported in related studies and literature.
The differential diagnosis mainly includes: 1. Metastatic choriocarcinoma: Since choriocarcinoma usually originates from the gonads and most of it metastasizes to the lungs, the diagnosis of PPC can only be made cautiously after excluding all gonadal lesions and other possible sites of choriocarcinoma. The patient underwent a series of thorough examinations after admission, and no tumor was found in other parts of the body, so the possibility of metastatic choriocarcinoma was ruled out. 2. Giant cell carcinoma that produces β-HCG, which has similar morphological characteristics to PPC. Although they all secrete beta-HCG, HCG-producing giant cell carcinomas have a strong immune response to TTF-1 because TTF-1 is an immunohistochemical marker of lung epithelial origin. In contrast, TTF-1 is negative in PPC. In this case, immunohistochemical staining showed HCG (+) and TTF-1 (-), and the diagnosis of PPC was reasonable. 3. SMARCA4-DUT, a newly discovered aggressive malignancy whose pathogenesis is still unknown. The most common sites for this tumor are the mediastinum, hilum, lungs, and pleura or chest wall. Smarca4-dut has undifferentiated or striated morphologic features and is disexpressed with SMARCA4, which can be used to assist in differential diagnosis by detecting blood β-HCG levels and using corresponding immunohistochemical markers. In this case, CT, ultrasound and other examinations found that no tumors were found in other parts of the patient except lung lesions. After surgery, blood β-hCG was still elevated due to tumor residue, and remained at a high level (>10000 mIU/mL) after chemotherapy. On the other hand, immunohistochemical results suggested that the tumor cells expressed HCG, were of germ cell origin (SALL4+, GATA3+ and TTF-1-), and the tumor cells were not expressing SMARCA4, so the diagnosis of primary pulmonary choriocarcinoma with SMARCA4 deletion was reasonable.
At present, the pathogenesis of primary choriocarcinoma of the lung is still unclear. Some researchers believe that it is caused by tumor transformation of ectopic primordial germ cells or spontaneous regression of occult primary gonadal tumors [10]. Other scholars believe that it may be caused by somatic cell derived tumor metaplasia or differentiation, similar to primary lung cancer through dedifferentiation into trophoblastic cells or choriocarcinoma [11]. In this case, after consultation with experts from the pathology Department of Shanghai Pulmonary Hospital, we tend to think that this tumor is the source of somatic cell tumor (non-small cell lung cancer) to the velvet cancer differentiation.
Male extrinsic primary choriocarcinoma is very rare and has a poor prognosis. Literature has studied 68 patients with PPC, including 36 males and 32 females, and found that the prognosis of male patients is worse than that of female patients. The median survival time of 68 patients is only 15 months, and the 1-year overall survival rate is 55.7% [12]. At present, there is a lack of effective treatment for this disease, and the traditional treatment is surgical resection combined with chemotherapy [13]. In recent years, with the approval of immune checkpoint inhibitors targeting programmed death receptor 1 (PD-1) and Programmed Death Ligand 1 (PD-L1) for the treatment of Non-Small Cell Lung Cancer (NSCLC), Multiple monoclonal antibodies can be used for immunotherapy of NSCLC. Foreign literature has reported the first successful treatment of a male PPC patient with postoperative recurrence using chemotherapy (carboplatin, paclitaxel) combined with immunosuppressants (nabuliumab, ipriimma), which may be an option for patients with advanced PPC [14]. In the prognosis assessment of 105 patients with SMARCA4-deficient NSCLC, it was also mentioned by researchers that immunotherapy combined with chemotherapy showed a longer median overall survival in these patients with distant metastases [15]. In addition, some scholars have suggested that chemotherapy combined with Immune Checkpoint Inhibitor (ICI) should be used as the preferred treatment for SMARCA4-deficient undifferentiated tumors of the lung [16]. According to the latest PD-L1 consensus guidelines, people with PD-L1 tumor cell expression levels ≥50% have more outstanding overall survival benefits using immunotherapy [17]. In this case, PPC patient was accompanied by SMARCA4 deletion. Despite 8 cycles of postoperative chemotherapy, multiple metastases in the whole body still appeared.
Although the expression level of PD-L1 was only 10%, considering that Tanaka et al. [18] also reported that a patient with only 10% PD-L1 expression received the combination treatment of first-line drugs with carboplatin, pemetrexed and pembrolizumab, and achieved partial remission. Whether this patient can also try chemotherapy combined with immune checkpoint inhibitors at a later stage to improve survival remains unknown. In addition, targeted therapy is currently a hot spot in tumor therapy. It has been reported in the literature that a male PPC patient underwent genetic testing after surgery, and mutations of Tumor Protein p53 (TP53), NRAS proto-oncogene (NRAS), and Fibroblast Growth Factor Receptor 1 (FGFR1) were found [19]. It is not yet clear how these genomic observations will impact future treatment options, and many genomic analyses are still at the basic or translational level of research, but in the future, more scholars should study the gene mutations and signaling pathways associated with PPC to improve such patient outcomes.
Conclusion
In summary, male primary pulmonary choriocarcinoma with SMARCA4 deletion is very rare, and the key to diagnosis is based on histological features combined with immunohistochemical findings, with reference to the patient’s blood β-HCG level. A patient needs to undergo a thorough examination to rule out metastatic choriocarcinoma of the lung and a range of other identifiable diseases before making a careful diagnosis. Despite the poor prognosis of the disease, it is still necessary to combine chemotherapy and immunosuppressive therapy after surgery to improve the survival rate of patients, and try to explore targeted therapies to benefit patients.
Acknowledgements: We would like to express our appreciation to the patient and his families and the experts consultation from the Pathology Department of Shanghai Cancer Hospital, Fudan University and Shanghai Pulmonary Hospital. This work was supported in part by funding from the Fund of Shanghai Municipal Health Commission (No. 202140099).
References
- Snoj Z, Kocijancic I, Skof E. Primary pulmonary choriocarcinoma, Radiol Oncol. 2016; 51: 1-7. [PubMed: 28265226]
- Zhang X, Ding B, Chen L, Huang X, Zhang K, et al. Primary pulmonary choriocarcinoma in male: report a case with genetic testing and review of the literature, Transl Cancer Res. 2022; 11: 1844-1849. [PubMed: 35836509]
- Peipei Zhu. One case of SMARCA4-deficient undifferentiated renal tumor, Chin J Pathology. 2023; 52: 299-301.
- Nambirajan A, Jain D. Recent updates in thoracic SMARCA4-deficient undifferentiated tumor, Semin Diagn Pathol. 2021; 38: 83-89. [PubMed: 34147303]
- Herpel E, Rieker RJ, Dienemann H, et al. SMARCA4 and SMARCA2 deficiency in non-small cell lung cancer: immunohistochemical survey of 316 consecutive specimens, Ann Diagn Pathol. 2017; 26: 47-51. [PubMed: 28038711]
- Nguyen HTT, Hoang HH, Le ATV. A Case Report of Primary Pulmonary Choriocarcinoma in a Man: Successful Combination of Surgery and Chemotherapy, Case Rep Oncol. 2020; 13: 923-928. [PubMed: 32884541]
- Shen Fei-yun, ZHAO Jin-kun, Zhang Hui-bo, et al. Clues and pitfalls of immunohistochemical diagnosis of pulmonary choriocarcinoma, Chinese Journal of Diagnostic Pathology. 2020; 27: 854-858.
- Huang Ben-xin, GUO Xiao-bo, Pan Hua-xin, et al. Expression and significance of transcription factor GATA3 in trophoblasts, Chinese Journal of Clinical and Experimental Pathology. 2016; 32: 652-655.
- Gasparri R, Sedda G, Brambilla D, Girelli L, Diotti C, et al. When a Differential Diagnosis is Fundamental: Choriocarcinoma mimicking lung carcinoma, J Clin Med, 2019; 8(11): 2018. [PubMed: 31752307]
- Zhu R, Jia C, Yan J, Luo Y, Huo Z. Primary pulmonary choriocarcinoma in a male that was successfully diagnosed and treated: A case report and review of the literature, Medicine (Baltimore). 2016; 95: e5693. [PubMed: 28033262]
- Onishi I, Kirimura S, Wakejima R, Okubo K, Odai T, et al. Primary pulmonary choriocarcinoma with a genomic sequence, Pathol Int. 2022; 72: 141-143. [PubMed: 34904768]
- Cao X, Feng H, Liu S, Chen L. Analysis of clinical characteristics and prognosis of 68 patients with primary pulmonary choriocarcinoma, BMC Pulm Med. 2023; 23: 75.[PubMed: 36890515]
- Johnson AM, Johnson CM, Khalil Z, Stitzel M, Teoh D. Case Report: Treatment of primary pulmonary choriocarcinoma with lung lobectomy and adjuvant chemotherapy, Gynecol Oncol Rep. 2022; 43: 101064. [PubMed: 36092979]
- Iso H, Hisakane K, Terashi N, Mikami E, Matsuki S, et al. A remarkable response to combination chemotherapy with nivolumab and ipilimumab in a patient with primary pulmonary choriocarcinoma: a case report, Transl Cancer Res. 2023; 12: 2212-2218.[PubMed: 37701113]
- Liang X, Gao X, Wang F, Li S, Zhou Y, et al. Clinical characteristics and prognostic analysis of SMARCA4-deficient non-small cell lung cancer, Cancer Med. 2023; 12: 14171-14182. [PubMed:37184108]
- Pokhrel A, Yadav R, Manvar KK, Wu R, Jaswani V, et al. Chemotherapy and Immune Checkpoint Inhibitors in a Case of SMARCA4-dUT: A Case Report and Review of Literature, J Investig Med High Impact Case Rep. 2023; 11: 23247096231176220. [PubMed: 37269109]
- Lung Cancer Group and Molecular Pathology Group of Cancer Pathology Committee of Chinese anti-Cancer Association, Lung Cancer Committee of Chinese anti-Cancer Association, Non-small Cell Non-cancer Committee of Chinese Society of Clinical Oncology. Chinese expert consensus on clinical testing of PD-L1 expression in non-small cell lung cancer (2023 version), Chin J Pathology. 2024; 53: 121-127.
- Tanaka S, Hayashi S, Isobe Y, Maruyama E, Ozawa H, et al. Positive outcome of first-line therapy for a SMARCA4-deficient thoracic sarcomatoid tumor, Int Cancer Conf J. 2021; 10: 112-115. [PubMed: 33786285]
- Zhang X, Ding B, Chen L, Huang X, Zhang K, et al. Primary pulmonary choriocarcinoma in male: report a case with genetic testing and review of the literature, Transl Cancer Res. 2022; 11: 1844-1849. [PubMed: 35836509]