Introduction
The conversion of leukemic cell phenotype or genotype during treatment is a rare occurrence, typically observed in infants and pediatric patients. Most commonly, cases with lineage switch from lymphoid to myeloid have been reported, and were frequently associated with t (4;11) (11q23) involving KMT2A rearrangement [1-7]. The underlying mechanism of lineage switch remains unclear. The phenomenon could result from clonal evolution, a pre-therapy sub-clone, or a new clone induced by therapy [8-12]. Herein, we present a unique case of an elderly patient who underwent lineage switch from B-Lymphoblastic Leukemia (B-ALL) to Acute Myeloid Leukemia (AML) after induction chemotherapy, subsequently changed to B- and myeloid Mixed Phenotype Leukemia (MPAL) following Azacytidine/Venetoclax. The patient was initially diagnosed B-ALL with KMT2A/AFF1 fusion gene. However, in the AML stage, the KMT2A/AFF1 abnormality disappeared, while ASXL1 mutation and RUNX1-RUNX1T1 fusion transcript were detected. Furthermore, when the patient’s leukemia changed to MPAL post AML regimen therapy, the KMT2A-AFF1 fusion gene re-appeared. To our knowledge this is the first reported case of an elderly patient whose leukemia started as B-ALL later switched to AML and then changed to MPAL during consecutive induction chemotherapy treatment.
Case presentation
A 65-year-old male presented to his primary care physician with bilateral lower extremity swelling and pain. Outpatient laboratory studies showed marked hyperleukocytosis with a White Blood Count (WBC) of 568 K/uL, anemia with a hemoglobin of 9.0 g/dL, thrombocytopenia with a platelet count of 45 K/uL, and with 87% blasts.
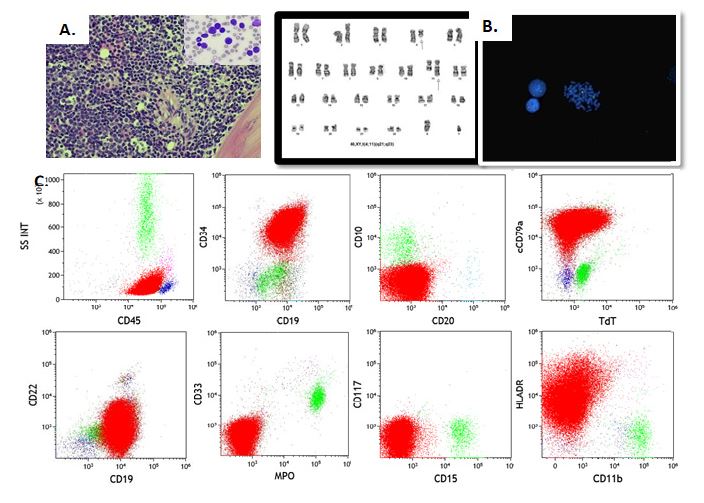
Peripheral blood and bone marrow flow cytometric analysis indicated an immunophenotype consistent with B-lymphoblasts. Bone marrow biopsy review showed hypercellular marrow and 92% blasts. Cytogenetics and FISH analysis revealed t(4;11)(q21;q23) forming KMT2A/AFF1 fusion gene (also known as MLL/AF4) (Figure 1).
Based on the findings, the patient was diagnosed with precursor B-cell Acute Lymphoblastic Leukemia (B-ALL) with KMT2A/AFF1. CNS involvement was seen on Cerebral Spinal Fluid (CSF) analysis. Induction chemotherapy with Vincristine/Dexamethasone followed by Hyper- CVAD regimen was started. Intrathecal alternating dose of cytarabine and methotrexate were administered according to protocol.
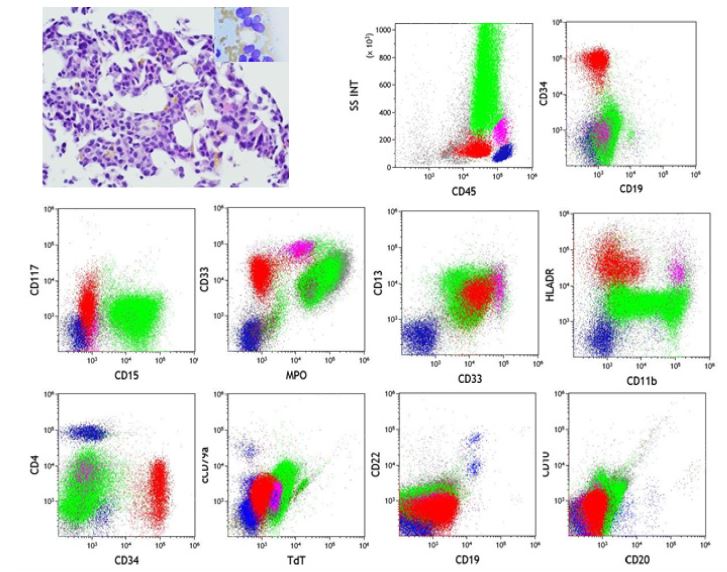
Two months later, he was noted to be persistently pancytopenic however 20% blasts were noted on the peripheral blood. Flow cytometric analysis of both peripheral blood and bone marrow showed aberrant myeloid blasts. Bone marrow morphology was consistent with lineage switch to Acute myeloid leukemia (Figure 2). Cytogenetic studies and FISH revealed a normal karyotype and no KMT2A/AFF1. ASXL1 mutation was detected by Next generation sequencing, along with RUNX1-RUNX1T1 fusion transcripts detected by RT-qPCR.
The therapy was changed to Azacytidine/Venetoclax, and the patient received two cycles. A follow up on day 30 post-therapy revealed a hypocellular marrow with no blasts; however, there was low level recurrence of KMT2A/AFF1 rearrangement detected by cytogenetics. Two months later, the patient experienced a relapse with 68% blasts characterized by the immunophenotype shown in (Figure 3). Briefly, the blasts expressed B-lymphoid lineage markers, including CD19, cCD79a, cCD22, TdT. Although the myeloid lineage marker MPO was not strongly expressed, the blasts also express CD15, CD65a and weak CD33. Given the cytogenetic finding of recurrent KMT2A/AFF1 fusion, a diagnosis of B/Myeloid mixed-phenotype acute leukemia was considered [13].
Blinatumomab salvage therapy was initiated, but complications arose with Cytokine Release Syndrome (CRS), requiring treatment with Tocilizumab and Dexamethasone. After discharge, the patient aspirated on food and was readmitted one day later for aspiration pneumonia complicated by septic shock, acute hypoxemic respiratory failure and hypoxic encephalopathy. Despite intubation and pressor support, the patient rapidly deteriorated, becoming bradycardic and hypotensive. The patient passed away 20 days after his most recent relapse and 181 days after initial diagnosis.
Discussion
In general, leukemic cells adhere to their lineage characteristics throughout the therapeutic process. Although rare, conversions of leukemic cell lineage (lymphoid or myeloid) have been reported, commonly in pediatric patients. The precise mechanism of lineage switches still remains unclear. One prominent proposed mechanism contributing to lineage switch is genetic mutations. Within the reported lineage switch cases the most strongly associated genetic mutations are those involving rearrangement of KMT2A(11q23) gene (KMT2Ar), specifically, t(4;11)(q21;q23) rearrangement with KMT2A/AFF1 fusion protein [14]. KMT2A/AFF1 is almost exclusively associated with B cell ALL, and is relatively rare in adult B-ALL compared to pediatric cases [6,15]. The presence of KMT2A/AFF1 may confer a higher degree of development plasticity to leukemia cells allowing the cells to transition between different lineages [9,16]. ASXL1 mutations have been frequently identified in various myeloid malignancies, including Myelodysplastic Syndrome (MDS) and Acute Myeloid Leukemia (AML), and are associated with poor prognosis [17-19]. There have been rare reported cases of MDS with ASXL1 mutations progress to Acute Lymphoid Leukemia (ALL) [20]. However, direct evidence of ASXL1 mutations involvement in AML or ALL lineage switch to mixed phenotype acute leukemia has not yet been reported.
In our case, the patient’s initial presentation was B-ALL with KMT2A/AFF1. After induction chemotherapy, lineage switched to AML with no KMT2A/AFF1, but ASXL1 mutation and RUNX1-RUNX1T1 fusion transcripts were detected. Although there have been incremental cases reported where CD19 targeted therapy induced lineage switch in acute B-lymphocytic leukemia, the lineage switch in our case occurred prior to Blinatumomab treatment. Induction chemotherapy itself does not directly induce specific genetic mutations like ASXL1 and/or RUNX1-RUNX1T1. We can speculate that there were two distinct leukemic clones in the initial presentation. The standard ALL chemotherapy regimens Vincristine/Dexamethasone may have led to the expansion of existing myeloid lineage subclone. After lineage switch from B-ALL to AML, post Azacytidine/Venetoclax treatment, the lineage conversion to B- and myeloid Mixed Phenotype Leukemia (MPAL) was also attributable to high leukemic plasticity associated with the KMT2A/AFF1 fusion gene. One of the important experiences gained from this case is that when a B-ALL case with KMT2A/AFF1 (or other KMT2A rearrangement) mutation is diagnosed, testing myeloid leukemia genetic panel including ASXL1, RUNX1-RUNX1T1, etc, might be beneficial.
Conclusion
In summary, the reported case with co-occurrence of KMT2A-rearrangement, ASXL1 mutation and RUNX1-RUNX1T1 fusion in the context of repeated lineage switch represents an extremely complex and challenging clinical scenario. This interplay between multiple genetic abnormalities underscores the dynamic nature of leukemia and the challenges it presents in clinical management. This case emphasizes the critical role of precise genetic characterization and individualized treatment planning in optimizing outcomes for patients with complex and evolving leukemia subtypes.
New findings
This report details a rare case of lineage switch in acute leukemia in an elderly patient. Initially diagnosed with B-ALL with KMT2A/AFF1, the patient’s leukemia transitioned to AML post- chemotherapy, lacking KMT2A/AFF1, and later evolved into MPAL with KMT2A/AFF1 upon relapse. The AML phase showed ASXL1 mutations and RUNX1-RUNX1T1 fusion. This indicates the pospossible emergence of distinct leukemic clones across phases, highlighting diagnostic and therapeutic challenges. The rapid transition suggests clonal selection by therapy or subclone evolution, underscoring the need for further investigation.
Declarations of interest: None.
Grants: This case report did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
- Ridge SA, Cabrera ME, Ford AM, Tapia S, Risueño C, et al. Rapid intraclonal switch of lineage dominance in congenital leukaemia with a MLL gene rearrangement. Leukemia. 1995; 9(12): 2023-6.
- Krawczuk-Rybak M, Zak J, Jaworowska B. A lineage switch from AML to ALL with persistent translocation t(4; 11) in congenital leukemia. Med Pediatr Oncol. 2003; 41(1): 95-6.
- Germano G, Pigazzi M, del Giudice L, Campo Dell’Orto M, Spinelli M, et al. Two consecutive immunophenotypic switches in a child with MLL-rearranged acute lymphoblastic leukemia. Haematologica. 2006; 91(5 Suppl): Ecr09.
- Chung HJ, Park CJ, Jang S, Chi HS, Seo EJ, et al. A case of lineage switch from acute lymphoblastic leukemia to acute myeloid leukemia. Korean J Lab Med. 2007; 27(2): 102-5.
- Trikalinos NA, Soupir CP, Dey BR. Lineage switch of acute lymphocyctic leukaemia with t(4; 11)(q21; q23) into acute myeloid leukaemia in an adult patient after allogeneic stem cell transplantation. Br J Haematol. 2009; 145(2): 262-4.
- Rossi JG, Bernasconi AR, Alonso CN, Rubio PL, Gallego MS, et al. Lineage switch in childhood acute leukemia: an unusual event with poor outcome. Am J Hematol. 2012; 87(9): 890-7.
- Balducci E, Nivaggioni V, Boudjarane J, Bouriche L, Rahal I, et al. Lineage switch from B acute lymphoblastic leukemia to acute monocytic leukemia with persistent t(4; 11)(q21; q23) and cytogenetic evolution under CD19-targeted therapy. Ann Hematol. 2017; 96(9): 1579-81.
- Sakaki H, Kanegane H, Nomura K, Goi K, Sugita K, et al. Early lineage switch in an infant acute lymphoblastic leukemia. Int J Hematol. 2009; 90(5): 653-5.
- Dorantes-Acosta E, Pelayo R. Lineage Switching in Acute Leukemias: A Consequence of Stem Cell Plasticity? Bone Marrow Research. 2012; 2012: 406796.
- Della Starza I, Ceglie G, Nunes V, Gianfelici V, Marinelli M, et al. A case of lineage switch from B-cell acute lymphoblastic leukaemia to acute myeloid leukaemia. Role of subclonal/clonal gene mutations. Br J Haematol. 2016; 174(4): 648-51.
- Rayes A, McMasters RL, O’Brien MM. Lineage Switch in MLL-Rearranged Infant Leukemia Following CD19-Directed Therapy. Pediatr Blood Cancer. 2016; 63(6): 1113-5.
- Haddox CL, Mangaonkar AA, Chen D, Shi M, He R, et al. Blinatumomab-induced lineage switch of B-ALL with t(4: 11)(q21; q23) KMT2A/AFF1 into an aggressive AML: Pre- and post-switch phenotypic, cytogenetic and molecular analysis. Blood Cancer J. 2017; 7(9): e607.
- George BS, Yohannan B, Gonzalez A, Rios A. Mixed-Phenotype Acute Leukemia: Clinical Diagnosis and Therapeutic Strategies.Biomedicines. 2022; 10(8).
- He RR, Nayer Z, Hogan M, Cuevo RS, Woodward K, et al. Immunotherapy- (Blinatumomab-) Related Lineage Switch of KMT2A/AFF1 Rearranged B-Lymphoblastic Leukemia into Acute Myeloid Leukemia/Myeloid Sarcoma and Subsequently into B/Myeloid Mixed Phenotype Acute Leukemia. Case Rep Hematol. 2019; 2019: 7394619.
- Meyer C, Burmeister T, Gröger D, Tsaur G, Fechina L, et al. The MLL recombinome of acute leukemias in 2017. Leukemia. 2018; 32(2): 273-84.
- Cuneo A, Balboni M, Piva N, Carli MG, Tomasi P, et al. Lineage switch and multilineage involvement in two cases of pH chromosome-positive acute leukemia: Evidence for a stem cell disease. Haematologica. 1994; 79(1): 76-82.
- Gelsi-Boyer V, Trouplin V, Adélaïde J, Bonansea J, Cervera N, et al. Mutations of polycomb-associated gene ASXL1 in myelodysplastic syndromes and chronic myelomonocytic leukaemia. Br J Haematol. 2009; 145(6): 788-800.
- Gelsi-Boyer V, Trouplin V, Roquain J, Adélaïde J, Carbuccia N, et al. ASXL1 mutation is associated with poor prognosis and acute transformation in chronic myelomonocytic leukaemia. Br J Haematol. 2010; 151(4): 365-75.
- Gelsi-Boyer V, Brecqueville M, Devillier R, Murati A, Mozziconacci MJ, et al. Mutations in ASXL1 are associated with poor prognosis across the spectrum of malignant myeloid diseases. J Hematol Oncol. 2012; 5: 12.
- Guo ZP, Tan YH, Li JL, Xu ZF, Chen XH, et alR. Acute pro-B-Cell lymphoblastic leukemia transformed from myelodysplastic syndrome with an ASXL1 missense mutation: A case report with literature review. Oncol Lett. 2018; 15(6): 9745-50.