Introduction
To first define a cancer patient, a cancer patient is a person who has received a cancer diagnosis who is: going to start treatment or receiving treatment for cancer or symptom management and/ or receiving palliative care [1].
Cachexia is a common manifestation in cancer patients. It is characterised by weight loss, loss of appetite, anemia and weakness [2].
Why are cancer patients so commonly malnourished?
It is estimated that between 30-85% of patients over 65 years with cancer suffer from malnutrition [3]. Furthermore 10-20% of oncology patients die from malnutrition itself [4]. The definition of insufficient nutritional intake is no food intake for 1 week or 60% reduction in required energy intake for 1-2 weeks [5].
There a number of reasons contributing to this. Firstly, cancer patients commonly have a reduced food intake either due to primary anorexia or other causes such as nausea, vomiting and mouth ulceration. Cancer also causes metabolic issues such as increased resting metabolic rate and insulin resistance. Furthermore cancer causes a systemic inflammatory syndrome, this results in accelerated breakdown of muscle and fat. These factors play a key role in the increased incidence of malnutrition and cachexia seen in cancer patients [1].
Weight loss in cancer patients is due to loss of fat and skeletal muscle in contrast to weight loss in non-cancer patients which is predominately due to loss of fat. Larger amounts of weight loss are directly correlated with reduced survival. Furthermore, weight loss greater than 10% combined with a reduction of food intake of more than 1500 kcal and a systemic inflammatory response are associated with a poorer prognosis [6].
Nutrition is a key component in the management of oncology patients. In a study conducted by Tong et al. 219 oncology patients receiving chemotherapy were assessed for nutrition impact symptoms. It was shown that patients who experienced nutrition impact symptoms, such as nausea and diarrhoea, experienced a lower quality of life and performance to treatment [7]. This highlights the importance of screening for malnutrition in oncology patients in order to optimise their treatment response and experience during treatment.
There are a number of approved methods for screening for malnutrition in oncology patients, such as Mini Nutritional Assessment (MNA), Malnutrition Universal Screening Tool (MUST), National Risk Screening 2002 (NRS 2002) and Malnutrition Screening Tool (MST). It is recommended that screening is performed at diagnosis and at regular intervals throughout the illness. With screening in place, it is hoped that patients who are at risk of malnutrition or are malnourished, are identified and referred to oncology nutritionists for early intervention [8].
Once these patients are referred they will first receive nutritional counselling, if this fails energy dense oral nutritional supplements can be prescribed. The final intervention would then be complete oral, parenteral or enteral nutrition. These interventions aim to prevent the catastrophic effects of malnutrition, including increased hospitalization, reduced response to cancer treatment, increased side effects in response to cancer treatment and poorer prognosis [9].
Another key component in the nutritional management of an oncology patient is counselling in relation to physical activity, this can reduce the accelerated breakdown of muscle [1].
As cancer is a common condition that is predicted to become more prevalent, there are estimations that 1 in 2 people will develop cancer by 2020 [10], and the incidence of malnutrition in these patients is between 30-85%, I chose to carry out an audit in STGH to investigate the incidence of malnutrition, I used the MNA to screen patients. This is a public health issue that has yet to be fully addressed in Ireland and I hope the results of this audit will highlight the unmet need for the nutritional management of oncology patients.
Methods
50 patients were assessed for malnutrition in South Tipperary General Hospital. Patients were assessed during their clinic visits, it was therefore only outpatients included in the audit.
Patients that were included were aged between 44 and 86 years, the median age was 64 years. 21 patients were male (42%), and 29 were female (58%). They all had solid organ tumors (breast, colon, lung, pancreas, ovarian, cervical, endometrial, renal cell) varying from stage 2-4. 47 patients (94%) were currently receiving chemotherapy and 3(6%) had received chemotherapy in the past month.
The patients nutritional status was assessed using the Mini Nutritional assessment. The MNA nutritional assessment involves 5 questions relating to reduction in food intake in the past 3 months, weight loss in the past 3 months, mobility and psychological issues including depression, acute stress and memory issues. Patients have three options for each question, answer options are generally in format: severe, moderate or not all. Patients BMI is also included in the assessment.
Each answer selected by the patient and patient’s BMI carries 0,1,2 or 3 points. Patients weight and height were measured by nursing staff and BMI subsequently calculated. Based on the number of points a patient receives they are categorized into 3 groups: normal nutritional status, at risk of malnutrition or malnourished.
Results
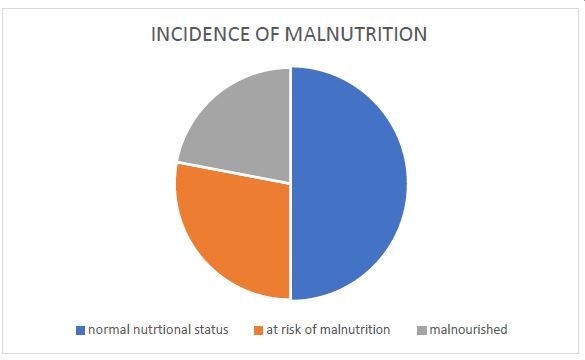
According to the results of the mini nutritional assessment it was shown that 25 of the 50 patients (50%) had a normal nutritional status, 14 patients were at risk of malnutrition (28%) and 11 patients were malnourished (22%).
The 11 patients in the malnourished category all had metastatic disease (colon, esophageal, rectal and cervical)
The 14 patients in the at risk category: 2 patients stage 3 colon, 1 patient stage 2 colon, 1 patient stage 3 jejunum, 1 patient pancreatic cancer, the other 9 patients had metastatic colon, ovarian, breast and lung cancer.
The 50 patients in the normal nutritional category: 1 patient stage 3 endometrial, 2 patients stage 3 rectal, 4 patients stage 3 colon, 1 patient inoperable cholangio carcinoma, 2 patients stage 3 lung cancer, 39 patients had metastatic colon, breast, prostate, renal cell carcinoma and rectal cancer.
A similar study was conducted in the Mercy hospital in Cork. In this study 432 oncology patients were audited using the MUST screening tool. According to the results of this, 36% of patients were at medium to high risk of malnutrition. These patients experienced higher a incidence of reduced quality of life, reduced appetite, nausea and vomiting. This further stresses the importance of screening for nutritional status [11].
The results of the study in mercy hospital and STGH are similar and would suggest that Irish oncology patients nutritional status is not being addressed sufficiently.
Discussion
The results of my audit suggest that it would be beneficial to screen all oncology patients for malnutrition regularly. According to the mini nutritional assessment 14 out of 50 patients were at risk of malnutrition. These patients would benefit from intervention to prevent them progressing to a malnutrition state. The 11 patients who are already malnourished will also need nutritional intervention.
It is worth noting that only 2 patients had a BMI that would indicate they were underweight, between 15-19.9. At present in South Tipperary general hospital it is current practice to record patients weight, height and BMI during their outpatients visits. The results of the MNA would suggest that BMI is not sufficient to identify all patients who are mal nourished. BMI has a number of recognised limitations including the fact that is a poor predictor of body fat percentage, it doesn’t take a person’s body build into consideration and it also doesn’t consider body fat location [12]. BMI is therefore not an accurate measurement for determining if someone if obese/normal weight or underweight so another method is necessary for identifying these patients.
I used the MNA to screen patients for malnutrition. The MNA was found to be the most sensitive tool in a comparative study conducted on 53 oncology patients. The study compared 3 nutritional screening tools: MNA, MST and MUST. The sensitivity of the tools were determined by comparing the number of patients the screening tools identified as malnourished to the number of patients an oncology nutritionist identified as malnourished during clinical assessment. The MNA was found to be the most sensitive, with a sensitivity of 92% [13].
Another study which screened 5334 elderly patients in community and nursing home settings, found the MNA to have a sensitivity of 98% in those >90 years, and 97% in those under 90years, the specificity was 44% and 52% respectively [14].
For this reason this appeared to be the most appropriate tool to use in my audit.
The aims of screening for malnutrition are to identify patients before they become malnourished and intervene early. The data is lacking on when is the optimal time to start nutritional intervention but the literature does state that it is very difficult to reverse the effects of malnutrition once they have taken hold, reiterating the importance of early identification of these patients and subsequent intervention [1].
In a systemic review and metanalysis of 5 RCTs, including 488 oncology patients, conducted by Halfdanarson et al. it was found that Nutritional counselling in malnourished patients improved patients quality of life [15]. In a similar study by Baldwin et al. 1414 patients received either nutritional counselling and or oral supplements. Out of the patients who received nutritional intervention only those receiving radiotherapy experienced an increased quality of life and weight gain, there was however no effects on survival time [16].
These studies show clear benefits at least in terms of quality of life for nutritional intervention in oncology patients.
The problem in Ireland at present is there are no enforced guidelines in relation to the nutritional management of oncology patients which means there is great variability between how patients are managed in each hospital. There are 40,000 people diagnosed with cancer each year in Ireland [17]. This clearly represents a huge public health issue if 20-80% of these patients are malnourished. In the Netherlands, there is a cost 2 billion euro each year due to disease related malnutrition, 300 million of which is spent on cancer related malnutrition [18].
The European Society for Clinical Nutrition and Metabolism (ESPEN) generated guidelines in 2016 for the nutritional management of oncology patients. These guidelines can be summarised by three main steps: step one is to screen all oncology patients for malnutrition, step two is to assess nutritional status more thoroughly by measuring food intake, body composition, markers of inflammation (CRP and albumin), resting energy expenditure and physical function and step three is to generate personalized nutritional intervention plans for each patient [4].
Guidelines for management of malnutrition have been established in other countries such as China, their guidelines can be summarised by ‘screen, intervene and supervene’. The guideline suggests screening using the MST, intervene if necessary with methods such as nutritional counselling, supplementation and lastly supervene by following up patients, for example providing patients with a post discharge nutrition plan [19].
These ESPEN guidelines are a good starting point but I believe for them to be enforced in all hospitals they need to be more specific. For example they should include what screening tool to use and set points for when intervention is necessary. Another issue with enforcing these guidelines is resources: a screening tool should be enforceable as most only take 2-3 minutes to complete, but the nutritional intervention will require a lot more input from nutritionists and this may not be possible in the number of Irish hospitals at present. As the cost of malnutrition is high, it would be beneficial to put more resources into preventing the development on malnutrition.
Conclusion
To conclude the oncology patients in STGH had a malnutrition rate of 22%. 28% of patients were at risk of malnutrition. As malnutrition has negative consequences in oncology patients, it would be beneficial to screen for same. The most sensitive tool for screening to date is the MNA. With screening in place patients can be identified early and receive early nutritional intervention to prevent them becoming malnourished.
Currently in STGH BMI is the ‘screening’ tool in use. Due to the results of this audit the oncology staff plan to implement screening all patients at monthly intervals using the MNA.
The rates of malnutrition will then be re-audited in one year.
References
- Arends, Jann, et al. ESPEN guidelines on nutrition in cancer patients Arends, Jann et al. Clinical Nutrition. 2017; 36: 11-48.
- Argilés JM, Busquets S, García-Martínez C, López-Soriano FJ. Mediators involved in the cancer anorexia-cachexia syndrome: Past, present, and future. Nutrition. 2005; 21: 977-85.
- Argiles JM. Cancer-associated malnutrition. Eur J Oncol Nurs. 2005; 9: S39-50.
- ESPEN expert group recommendations for action against cancer-related malnutrition Arends, J. et al. Clinical Nutrition. 36: 1187- 1196.
- Arends J, Bachmann P, Baracos V, Barthelemy N, Bertz H, et al. ESPEN guidelines on nutrition in cancer patients. Clin Nutr. 2017; 36(1): 11e48.
- Dhanapal R, Saraswathi T, Govind RN. Cancer cachexia. Journal of Oral and Maxillofacial Pathology: JOMFP. 2011; 15(3): 257-260.
- Tong H, Isenring E, Yates P. Support Care Cancer. 2009; 17: 83.
- Caccialanza R, Pedrazzoli P, Cereda E, et al. Nutritional Support in Cancer Patients: A Position Paper from the Italian Society of Medical Oncology (AIOM) and the Italian Society of Artificial Nutrition and Metabolism (SINPE). Journal of Cancer. 2016; 7(2): 131-135. doi:10.7150/jca.13818.
- Cushen S, Power D, Mc Eneaney P, Daly L, Ryan A. A prospective investigation into the nutritional status of Irish oncology outpatients: Prevalence of malnutrition, cachexia, sarcopenia and impact on quality of life. Proceedings of the Nutrition Society. 2015; 74(OCE2): E159.
- xhttps://www.cancer.ie/about-us/media-centre/cancer- statistics#sthash.K0PNuhBH.dpbs
- Nuttall FQ. Body Mass Index: Obesity, BMI, and Health: A Critical Review. Nutrition Today. 2015; 50(3): 117-128.
- Roulston F, McDermott R. Comparison of three validated nutritional screening tools in the oncology setting. Proceedings of the Nutrition Society. 2008; 67(OCE7): E260.
- Vandewoude M, Van Gossum A. J Nutr Health Aging. 2013; 17: 310.
- Arends Jann, et al. ESPEN guidelines on nutrition in cancer patients Arends, Jann et al. Clinical Nutrition. 2017; 36: 11-48.
- Halfdanarson TR, Thordardottir E, West CP, Jatoi A. Does dietary counselling improve quality of life in cancer patients? A systematic review and meta- analysis. J Support Oncol. 2008; 6: 234-237.
- Baldwin C, Spiro A, Ahern R, Emery PW. Oral nutrition therapy in malnourished patients with cancer: a systematic review and meta-analysis. J Natl Cancer Inst. 2012; 104: 371-385
- https://www.mariekeating.ie/cancer-information/cancer-in-ireland/
- K Freijer, SS Tan, MA Koopmanschap, JM Meijers, RJ Halfens, et al. The economic costs of disease related malnutrition Clin Nutr. 2013; 32(1): 136-141.
- Correia MI, Hegazi RA, Higashiguchi T, Michel JP, Reddy BR, et al. Evidence-based recommendations for addressing malnutrition in health care: an updated strategy from the feed M.E. Global Study Group. J Am Med Dir Assoc. 2014; 15: 544e50