Introduction
The most common salivary gland tumor is the parotid tumor and represents between 80-85% of all salivary gland tumors in general. Approximately 75-85% of parotid tumors are benign and 25-20% are malignant.
Salivary gland tumors represents approximately 3% to 6% of all head and neck tumors. With an overall incidence of 0.4-13.5 cases per 100,000 people and mortality of 650 patients per year in the United States, the age of presentation between 55 and 64 years of age [1,3].
In the development of parotid gland cancer there are not predominant factor associated, several factors have been implicated as potential causes: Radiation exposure, Epstein Barr virus infection (associated with lymphoepithelial carcinoma), and industrial exposure [2].
The clinical presentation usually begins with an increase volume of the gland, generally painless, the presence of pain or facial nerve involvement (example: facial nerve palsy) generally indicative a malignant tumor. High-grade tumors spread to regional lymph nodes, more frequency cervical node levels I, II, and III [4].
The most frequent malignant histological type of the parotid gland is mucoepidermoid (35%), the cystic adenoid (10 to 15%) is important to mention because has an affinity for neural invasion [5,6].
Complete surgical resection is the most important treatment. The patients considered for adjuvant radiotherapy presented the following histopathological factors: Tumor T3-4, lymph node invasion positive, lymphovascular invasion positive, neural invasion positive, perineural invasion positive, positive margin, close margin positive, histology high grade and histology cystic adenoid [7,8].
The 5-year survival by clinical stage are: I - 96%, II - 77%, III - 73%, and IV - 37% [9].
The follow up is necessary to detect early relapses and detect complications. Patients should be educated about the possible signs and symptoms of recurrence as dysphonia, pain, dysphagia, bleeding, and palpable lymph nodes.
In patients with malignant parotid gland tumors the follow up is important into the first four years, because approximately 80 to 90% of all recurrences occur in this time. Continuous monitoring is suggested by the risk of recurrence beyond five years. Distant metastases can occur in 17% and are more frequently located at the lung, bone and liver. In cystic adenoid tumors, distant metastases can occur 10 to 20 years after the end of treatment [1,10].
The objective of this study was evaluating the benefit in local control at two years in patients with diagnosis of parotid gland cancer who received adjuvant radiotherapy.
Material and methods
We reviewed the expedients of patients diagnosed with parotid cancer treated the Oncology Hospital XXI century between 2013 and 2018 to obtained: age, sex, date of surgical resection, histopathological report (tumor size, lymph node invasion, lymphovascular invasion, neural invasion, perineural invasion, margin, close margin, histological grade and histological type), initiation date of radiotherapy, date of last radiotherapy session, dose and radiotherapy technique used. Local control was defined as: no evidence clinical and radiological of the disease measured from the surgical resection at two years.
The evaluation of tumor size was measured with the TNM classification from AJCC 8th edition of 2017, and the close margin positive was determined when was less than 5 mm (distance from the surgical edge the tumor) [11].
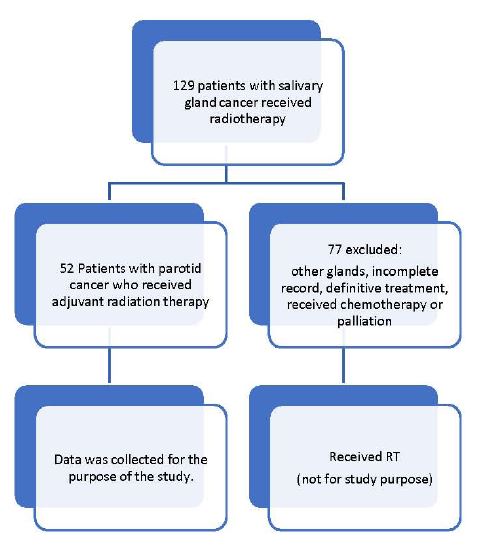
Were 129 patients with cancer of salivary gland who received radiotherapy, 77 patients were excluded for different reasons as: radiation of another salivary gland, incomplete medical record, receiving single treatment with radiotherapy, received chemotherapy or palliative treatment. Were evaluated 52 patients with parotid cancer who received adjuvant radiation therapy (Image 1).
Table 1: Demographic and clinical characteristics.
| CHARACTERISTICS |
# PATIENTS (%) |
| Ages |
| <55 |
30(57.7) |
| >55 |
22(42.3) |
| Sex |
| Women |
26 (50) |
| Men |
26(50) |
| Size tumor(T) |
|
| T1 |
6(11.5) |
| T2 |
27(51.9) |
| T3 |
16(30.8) |
| T4 |
3(5.8) |
| Lymph nodeinvasion |
|
| Negative |
25(48.1) |
| Positive |
27(51.9) |
| Histological grade |
|
| G1 |
15(28.8) |
| G2 |
15(28.8) |
| G3 |
22(42.3) |
| Lymphovascular invasion |
| Negative |
35(67.3) |
| Positive |
17(32.7) |
| Margin |
| Negative |
30(57.7) |
| Positive |
22(42.3) |
| Close margin |
| Negative |
32(61.5) |
| Positive |
20(38.5) |
| Histological type |
| Mucoepidermoid |
20(38.5) |
| Cystic adenoid |
5(9.6) |
| Acinar cells |
10(19.2) |
| Polymorphic adenocarcinoma |
3(5.8) |
| Clear cells |
2(3.8) |
| Basal cells |
0(0) |
| Others |
12(23.1) |
| Neural invasion |
| Negative |
44(84.6) |
| Positive |
8(15.4) |
| Perineural invasion |
| Negative |
41(78.8) |
| Positive |
11(21.2) |
| Dose RT |
| <66Gy |
36(69.2) |
| >66Gy |
16(30.8) |
| Technique RT |
| 3D |
23(44.2) |
| VMAT |
29(55.8) |
| Begin RT |
| Before weeks 23 |
32(61.5) |
| After weeks23 |
20(38.5) |
Results
We analyses 52 patients with parotid gland cancer who received adjuvant radiotherapy from January 2013 to December 2018. There were 26 men and 26 women, 42.3% was younger than 55 year, mean of 56; tumor size: T1 - 11.5%, T2 - 51.9%, T3 - 30.8% and T4 - 5.8%; lymph node invasion positive 51.9% and negative 48.1%; histological grade: G1 - 28.8%, G2 - 28.8% and G3 - 42.3%; lymphovascular invasion positive 32.7% and negative 67.3%; positive margin 42.3% and negative 57.7%: near margin positive 38.5% and negative 61.5%.
The histology was: mucoepidermoid 38.5%, cystic adenoid 9.6%, acinar cells 19.2%, pleomorphic adenocarcinoma 5.8%, clear cells 3.8% and other 23.1% (lymphoepithelial, salivary duct carcinoma, myoepithelial carcinoma, mixed malignant tumor, expleomorphic adenocarcinoma and unspecified adenocarcinoma). Neural invasion positive 15.4% and negative 84.6%; perineural invasion positive 21.2% and negative 78.8%. Radiotherapy doses; less than 66Gy represent 69.2% and who received greater than 66Gy 30.8% (average of 62.19Gy) The VMAT radiotherapy technique was 55.8% and 3D was 44.2%; the initiation of radiotherapy before than 23 weeks after surgery was 61.5% and after than 23 weeks was 38.5% (median of 22 weeks).
Demographic characteristics of the population are showed in table 1.
Table 2: Multivariable cox regression for local control.
| VARIABLE |
HR |
RANGE |
P |
| Ages <55 |
1 |
|
|
| Ages >55 |
0.88 |
0.32 – 2.38 |
0.80 |
| Women |
1 |
|
|
| Men |
0.91 |
0.34 – 2.45 |
0.86 |
| T1 Y T2 |
1 |
|
|
| T3 Y T4 |
3.83 |
1.38 – 10.60 |
0.01 |
| Lymph node invasionnegative |
1 |
|
|
| Lymph node invasion positive |
0.96 |
0.36 – 2.60 |
0.95 |
| Grade 1 Y 2 |
1 |
|
|
| Grade 3 |
3.97 |
1.34 – 11.71 |
0.01 |
| Lymphovascular invasion negative |
1 |
|
|
| Lymphovascular invasion positive |
1.78 |
0.66 – 4.79 |
0.25 |
| Margin negative - |
1 |
|
|
| Margin positive + |
1.54 |
0.57 – 4.19 |
0.38 |
| Close marginnegative |
1 |
|
|
| Close marginpositive |
0.61 |
0.21 – 1.78 |
0.37 |
| Neural invasion negative |
1 |
|
|
| Neural invasion positive |
3.60 |
1.22 – 10.63 |
0.02 |
| Perineural invasion negative |
1 |
|
|
| Perineural invasion positive |
2.81 |
1.01 – 7.80 |
0.04 |
| Before weeks23 |
1 |
|
|
| After weeks23 |
2.835 |
1.026-7.833 |
0.04 |
| Dose <66GY |
1 |
|
|
| Dose >66GY |
0.843 |
0.270-2.627 |
0.84 |
| Technique 3D |
1 |
|
|
| Technique VMAT |
0.775 |
0.287-2.091 |
0.61 |
| Mucoepidermoid |
1 |
|
|
| Cystic adenoid |
2.207 |
0.526-9.258 |
0.85 |
| Acinar cells |
0.0 |
0.0-7.21 |
0.96 |
| Polymorphic adenocarcinoma |
1.388 |
0.161-11.952 |
0.76 |
| Clear cells |
2.187 |
0.254-18.839 |
0.47 |
| Others |
2.088 |
0.636-6.848 |
0.22 |
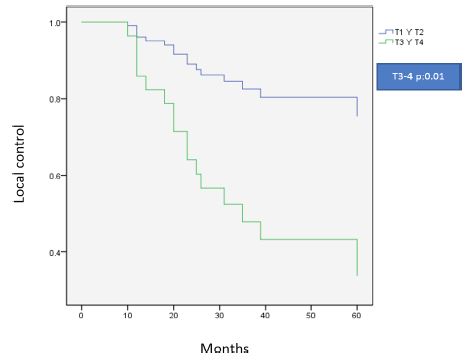
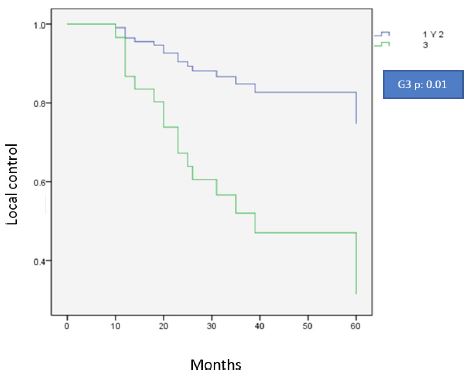
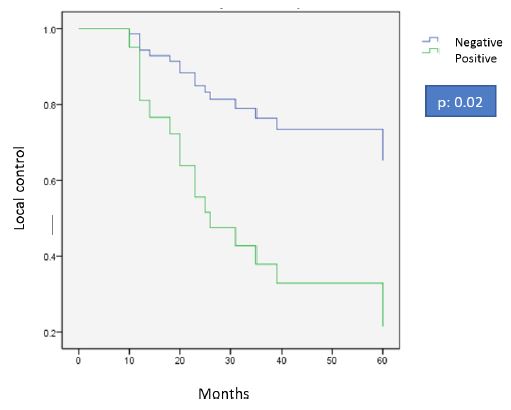
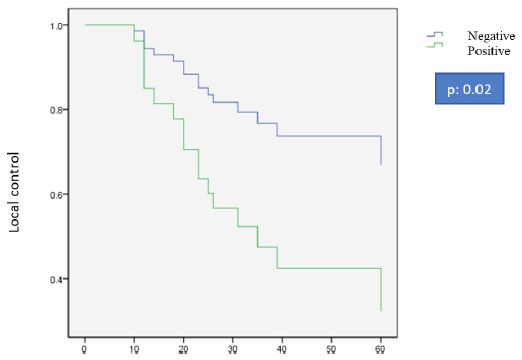
In the multivariate Cox analysis (Table 2) the factors that decrease local control and had significant difference were: tumor size T 3-4 [HR 3.83 (95% CI, 1.38-10.60, p 0.01)], histologic grade 3 [HR 3.97 (95% CI, 1.34-11.71, p 0.01)], positive neural invasion [HR 3.60 (95% CI 1.22-10.63, p0.02)], positive perineural invasion [HR 2.81 (95% CI, 1.01-7.80, p 0.04)] and begin the radiotherapy after week 23 [HR 2,835 (95% CI, 1,026-7,833, p 0.04)] (Figures 1-5).
The other factors such: radiotherapy technique (VMAT and 3D), radiation dose (< 66 Gy and > 66 Gy), lymph node invasion, close margin, positive margin, histology, sex and age have no significant difference.
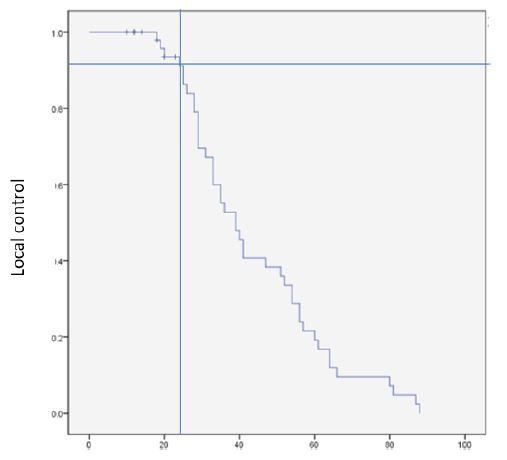
Local control at two years was 92% by Kaplan Meier. Of the 52 patients evaluated 10 had disease recurrence in less than 24 months (Figure 6).
The patients with recurrence has these characteristics: more 55 years (70%); men (60%); lymph node invasion positive (50%); grade 3 (70%); lymphovascular invasion positive (40%); positive margin (50%); close margin positive (20%); the most frequent histology was mucoepidermoid (40%); neural invasion positive (30%); perineural invasion positive (30%); begin of radiation after weeks 23 (50%); the radiation dose more than 66Gy (40%) and VMAT technique (60%).
Recurrence was observed local in 8 patients and local / distance (lung) in 2. 4 deaths were observed that had at least one of the adverse factors.
Discussion
The local control was measured at two years in patients with parotid cancer with adjuvant radiotherapy, 52 patients were select in a period from 2013 to 2018, of these 10 patients recurred at 2 years.
Chris H. J. Terhaard in 2005 evaluated patients with salivary gland cancer, compared the role of adjuvant radiotherapy versus surgery alone or radiotherapy as definitive treatment in unresectable tumors and concluded that adjuvant radiotherapy was indicated when the patients presented the following factors: T3-4 tumor, incomplete resection, close margin, bone invasion, perineural invasion and lymph nodes positive.
Adjuvant Radiation dose was established >60 Gy and primary treatment doses >66 Gy.
Also evaluated the time to receive adjuvant radiotherapy from week 6 to 12 and there was no significant difference, this study has a great importance, because it demonstrated some of the indications for adjuvant radiotherapy and dose.
Another study by Michele Nagliati (2015), evaluated the role of adjuvant radiotherapy versus surgery alone in patients with parotid gland cancer, described that only factor it mattered for recurrence was the clinical stage T3.
From Korea in 2016 by Jae-Keun Cho evaluated adjuvant radiotherapy versus surgery alone, report some factors for recurrence such as lymph node invasion positive, clinical stage T3-4 and positive margin [12-14].
The three studies mentioned that the clinical stage T3-4 is important factor for recurrence.
Chris H. J. Terhaard (2005) described the perineural invasion had a significant difference as a factor for recurrence.
Jae-Keun Cho and Chris h. J. Terhaard reported the importance factors for recurrence such as the lymph node invasion positive, positive margin and close margin, however in this study there was no significant difference.
The study by Chris h. J. Terhaard evaluated the start of adjuvant radiotherapy from week 6 to 12 and showed no significant difference, however, in our study was two groups: the first less than week 23 and the second more week 23, there is a statistically significant difference regarding the time to start adjuvant radiotherapy, starting adjuvant radiotherapy less of week 23 will offer better local control at two years.
In this study, different from the reported in the literature, grade 3 and the neural invasion positive had a significant difference, so they are factors for recurrence.
Local control has been reported in literature was 89.6% at 10 years, in our center we reached 92% at 2 years [12-14].
Conclusion
Patients with parotid cancer who received adjuvant radiotherapy had a local control at two years of 92%.
Associated factors with less local control were: T3-4, grade 3, neural invasion positive, perineural invasion positive and initiating adjuvant radiation more of week 23.
Previously in the literature, it was reported that the time to start adjuvant radiotherapy did not have a significant difference since the initiation of radiotherapy was only evaluated at weeks 12 postoperatively, patients who started adjuvant radiotherapy in our study less weeks 23 were observed to have better local control vs those who started more than weeks 23.
References
- Deschler DG, Emerick KS, Wirth JL, Busse PM. Head and neck cancer a multidisciplinary approach fourth edition 2014 Philadelphia, Chapter 25 management of salivary gland tumors. 2014; 697-699: 715-717.
- Perez CA, Brady LW, Halperin EC, et al. Perez and Bradys Principles and practice of Radiation Oncology, Seventh Edition. Philadelphia Chapter 46 Salivary Gland. 2018; 3011-3038.
- Scott AL. Salivary gland tumors: Epidemiology, diagnosis, evaluation, and staging. 2019.
- Hansen EK, Roach III M. Handbook of Evidence-Based Radiation Oncology 3rd Edition Springer San Francisco California. Chapter 10 Salivary Gland Tumors. 2018; 229.
- Guzzo M, Locati LD, Prott FJ, et al. Major and minor salivary gland tumors. Crit Rev Oncol Hematol. 2010; 74: 134.6.
- El-Naggar AK, Chan JKC, Grandis JR, et al. World Health Organization Classification of Tumours of Head and Neck, IARC, Lyon. 2017.
- Wang X, Luo Y, Li M, Yan H, Sun M, et al. Management of salivary gland carcinomas - a review. Oncotarget. 2016; 8(3).
- National Comprehensive Cancer Network versión 3.2019, Head and Neck Cancers, Salivary gland Tumors. 2019; 81-85.
- Kimberley Ho, Helen Lin. Salivary Gland Cancer Overview. Ho et al. Head & Neck Oncology. 2011; 3: 40
- Scott A Laurie, Bradley Schiff. Malignant salivary gland tumors: Treatment of recurrent and metastatic disease, Up To Date. 2017.
- Lydiatt WM, Patel SG, O’Sullivan B, et al. Head and Neck cancers-major changes in the American Joint Committee on cancer eighth edition cancer staging manual. Chicago, CA Cancer J Clin. 2017; 67: 122.
- Terhaard CH, Lubsen H, Rasch CR, Levendag PC, Kaanders HH, et al. The role of radiotherapy in the treatment of malignant salivary gland tumors; Dutch Head and Neck Oncology Cooperative Group 2005 Netherlands. 2005; 61(1):103-11.
- Michele Nagliati1, Andrea Bolner. Surgery and radiotherapy in the treatment of malignant parotid tumors: a retrospectivemulticenter study, Italia. 2015.
- Jae-Keun Cho, Byung-Woo Lim. Low-Grade Salivary Gland Cancers: Treatment Outcomes, Extent of Surgery and Indications for Postoperative Adjuvant Radiation Therapy, Korea. 2016.