Introduction
Rapid advancements in cancer radiotherapy, particularly in image-guidance techniques and real-time adaptive radiation therapy techniques, as well as revolutionary changes in medical physics dose prescription methods have enabled the provision of highly accurate and minimally invasive radiotherapy suitable for a wide variety of pathological conditions [1].Rapid advancements in cancer radiotherapy, particularly in image-guidance techniques and real-time adaptive radiation therapy techniques, as well as revolutionary changes in medical physics dose prescription methods have enabled the provision of highly accurate and minimally invasive radiotherapy suitable for a wide variety of pathological conditions [1].Rapid advancements in cancer radiotherapy, particularly in image-guidance techniques and real-time adaptive radiation therapy techniques, as well as revolutionary changes in medical physics dose prescription methods have enabled the provision of highly accurate and minimally invasive radiotherapy suitable for a wide variety of pathological conditions [1].
In this context, nurses play an essential role by quickly assessing patients’ conditions, providing decision support for treatment options, managing adverse events, and promoting self-care post-treatment [2]. Specifically, nurses offer medical counseling and guidance to help patients acquire self-care skills to address the physical, mental, and social effects of treatment and the decline in quality of life associated with cancer progression. It is essential that patients receive guidance from nurses and acquire the necessary skills and knowledge before or during hospital visits for radiation therapy, which typically extends over several weeks. Therefore, it is important for both patients and medical staff to record the details of radiotherapy and progress post-treatment, and for patients to have a Radiotherapy Notebook [3] that can be shared with medical staff anywhere and at any time.
However, a previous literature review [4] indicated the need to develop common indicators that can be used by both patients and nurses to establish effective nursing care and symptom management. Another literature review [5] concluded that, for patients to receive outpatient radiotherapy while continuing to work, it is essential that hospital nurses, workplace nurses, and other related personnel collaborate in understanding and advocating for the patient’s wishes. Providing appropriate teaching, guidance, and knowledge to cancer patients can substantially affect their quality of life. Therefore, we believe that patients require long-term support to balance work and rest, and to live and work with their illness.
Our aim was to develop an information-gathering tool to support patients undergoing outpatient radiation therapy. Such a tool would enable patients and nurses to use a common method to assess symptom management, identify potential physical and psychological reactions and social effects during outpatient radiation therapy based on the patient’s pre-treatment background, identify patients’ concerns and questions early on, and support patients trying to balance work and treatment. The tool could facilitate support for patients who are balancing work and medical treatment.
To obtain data to inform the development of the information-gathering tool, we conducted three studies: two survey studies and an interview study. First, a retrospective survey of patients who had completed outpatient radiation therapy was conducted to identify the factors that enabled patients to continue their therapy. Next, an information-gathering tool that assessed these factors was distributed to patients in advance, and they were asked to complete it.
The information-gathering tool was then used to conduct interviews on the decision-making process from cancer diagnosis to the selection of outpatient radiation therapy, explanations to family and workplaces, advantages and challenges of treatment while working, experiences and innovations during treatment, support from workplace and family, and future aspirations. The study aim was to identify factors that contribute to the continuation of outpatient radiation therapy. The tool also included a free-text field for qualitative data; this permitted the analysis of individual situations and responses to identify factors that enable patients to persist with their treatment.
Methods
The following studies were conducted to obtain information for the development of the information-gathering tool.
Survey study I
Definition of terms
1. In this paper, “young nurses” refers to nurses estimated to have reached the “competent” or “proficient” levels in Benner’s five levels of skill acquisition in clinical nursing practice [6], and who had 2 to 5 years of experience.
2. The term “radiation therapy” is used to describe three types of therapy: External-beam irradiation, sealed-source radiation, and internal radiation. External irradiation is the most commonly used type of radiation therapy. In this study, the term “radiation therapy” refers only to external irradiation therapy.
Study I
Six randomly selected cancer patients who, while working, received and completed their first radiation therapy at an outpatient clinic at University Hospital A between January and June 2017 participated. We analyzed previous literature reviews [4,5] to identify and synthesize factors related to patients’ continuation of outpatient radiation therapy. We developed two questionnaires, the Radiation Therapy Information Sheet (RT sheet) and the Patient Basic Information and Social Factors Information Sheet (BI sheet) to identify any additional information. The BI sheet assessed general demographic, clinical, and social factors. The RT sheet evaluated specific details related to the patients’ radiation therapy, including treatment schedules, side effects, and adherence to therapy.
Survey study II
Questionnaire survey: Participants were 14 cancer patients who, while working, received their first radiation therapy at an outpatient clinic at University Hospital A and University Hospital B during the survey period and who agreed to participate in the research. As the purpose of the survey was to identify factors that enable patients to continue outpatient radiation therapy, we included both patients who were working and those on a leave of absence. The rationale for these modifications was that as treatment progresses, tumor size changes, which in turn affects the number of treatments required. Thus, it was necessary to adjust the questions to accurately reflect these dynamics and their impact on the patient’s treatment regimen. Additionally, a new information sheet, the Symptoms and Physical Condition Sheet (SP sheet), was introduced to evaluate the patient’s condition on the day of radiation therapy. The researcher obtained information from patients’ medical records for the RT sheet, and the BI and SP sheets were distributed to participants to complete in advance.
The SP sheet included the following items:
Are you getting enough rest?, Are you getting enough sleep?, Describe yourself today (PS: physical status), Are you currently experiencing any symptoms? These items were used to assess patients’ condition on the day of radiotherapy.
Study III
Interview study: An interview study was conducted with seven patients from Survey Study II who agreed to participate.
The BI and SP sheets were distributed to participants to complete in advance.
The interviews were approximately 1 hour per person.
The researcher reviewed the completed BI and SP sheets during the interview.
The researcher reviewed the completed BI sheets during the interview. Interview content included the process of choosing outpatient radiation therapy, communication about the illness and treatment with family and workplaces, advantages and challenges of receiving treatment while working, experiences and thoughts during treatment, support received from workplace and family, and future hopes.
First, we documented, summarized, and confirmed participants’ statements. The interview summaries were coded into meaningful units. The codes were examined for commonalities and differences, classified, and subcategories were created. These subcategories were aggregated into categories. The coresearchers discussed the relationships between the categories.
Analysis of free-form responses from the BI sheet
The free-form responses from all 14 patients in Survey Study II were extracted and summarized. These summaries were coded into meaningful units. The codes were examined for commonalities and differences, and then classified. These classifications were aggregated into categories. The coresearchers discussed the relationships between the categories.
Creation of a draft information-gathering tool
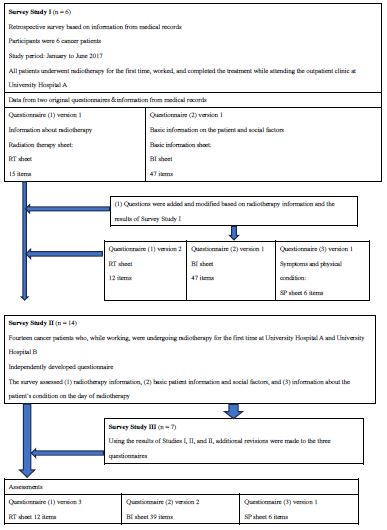
A draft information-gathering tool: The responses on the BI and SP sheets from the 14 participants in Survey Study II and the 7 participants in Study III were analyzed and examined by the coresearchers. Additionally, feedback was obtained from nurses familiar with radiation nursing and those involved in radiation therapy at University Hospital A and University Hospital B, and revisions were made accordingly. The process of creating the draft information-gathering tool is shown in Figure 1.
Statistical analysis
To verify the practical usefulness of the developed information-gathering tool, we aimed to analyze the relationships between the items on the BI sheet. By doing so, we sought to determine whether the tool effectively captures the necessary information to support patient care during outpatient radiation therapy. Given the sample size of 14, we acknowledge that some items may not be statistically testable. However, we utilized Spearman’s rank correlation coefficients to explore the associations between variables, supplemented by 95% confidence intervals. For items with strong significant correlations, we performed a chi-squared test using cross-tabulation. The limited sample size does constrain the generalizability of the findings, but this analysis serves as an initial step in evaluating the tool’s potential effectiveness. SPSS analysis software (IBM Corp., Armonk, NY, USA) Ver 28.0.1 was used for the analysis.
Ethical considerations: This research was conducted after obtaining approval from the Ethical Review Committee of Kagoshima University Hospital, Faculty of Medicine and Dentistry (Reception No.: 170136 Epidemic-Revision 2). Additionally, approval was obtained from the Ethical Review Committee of Nagasaki University Hospital (Reception No.: 18052116 Epidemic-Revision 2). Participants received written explanations of the questionnaire surveys and the questionnaires were self-administered and anonymous. Participation was voluntary. Consent for the study was deemed to have been obtained upon response. To fully protect participants’ privacy, the surveys contained no questions that could identify individuals. Any presentation and/or publication of the survey results will use aggregated data, and no information that could identify individuals or their group affiliation will be disclosed. During the study period, we took the utmost care to protect participants’ information by storing materials containing response data and group information in a locked storage room. After completion and publication of the research, all computer data will be permanently erased, all paper-based materials containing group information will be shredded and destroyed, and voice data will be deleted.
Results
Results of survey study I and revision of the questionnaire
Background participant information: The clinical diagnoses of the six participants comprised breast cancer (1), parotid cancer (1), and prostate cancer (4). Five subjects had received both radiation therapy and hormone therapy. (Table 1) shows background information for the participants.
Revision of the RT sheet
Two questions were added to the RT sheet: “Treatment method before receiving radiotherapy” and “Whether the patient received that treatment at their own facility or at multiple facilities.”
Results of survey study II
1) Basic participant information
The ages of the 14 participants ranged from 24 to 68 years, with a mean age of 56.93 years. Clinical diagnoses were as follows: breast cancer (n=7), eye tumor (n=1), laryngeal cancer (n=1), prostate cancer (n=2), colon cancer (n=2), and malignant lymphoma (n=1).
2) BI sheets
(Table 3) presents a tabulation of the survey items on the SP sheet for the 14 participants.
Results of survey study III
Results of interviews: The clinical diagnoses of the seven interviewees comprised breast cancer (n=1), eye tumor (n=1), laryngeal cancer (n=1), colorectal cancer (n=1), and prostate cancer (n=2). (Table 2) provides participant background information. The analysis of the interview data identified four categories (Table 4).
Decision-making process
Many participants sought opinions from a variety of sources, including family, work, patient groups, and online information. Patient groups and online information exchanges played a particularly important role in treatment decisions.
Experiences during treatment
Balancing treatment and work was a major challenge, requiring time management, fatigue management, and symptom adjustment. Participants showed flexibility in adjusting their treatment schedules and cooperated closely with their healthcare providers.
Support and resources
Support from the workplace varied substantially. Emotional support from family members was noted, but there were few specific instances of tangible support.
Information and support networks
Patient and family associations served as sources of knowledge, but their use was limited. Online platforms were highly valued as useful sources of information.
Analysis of free-form questionnaire responses
Participants were asked to provide free-form responses on the BI sheet about the following factors that improved their ability to continue with treatment: personal efforts they were making, any allowances made by their workplace, measures taken to ensure they could continue working and receiving treatment, and family support (Table 5). The # symbol in the table indicates responses from patients on leave. Responses from five patients on leave and nine patients who were still working were compared. The following categories were identified.
Engagement in activities other than treatment
Activities participants engaged in included diet and nutrition, physical activity and exercise, relaxation and rest, daily routines, and health monitoring (Table 5). Patients managed their health by refreshing their body and mind through relaxation and rest, and by creating daily routines.
Making an effort in daily life
Time management and efficiency were frequently mentioned. Patients managed their time efficiently, balancing their work duties while also taking care of their family and roommates.
Allowances made by the workplace during treatment
Patients mentioned changes to working hours, work responsibilities, support for absences, and special allowances for medical treatments. Workplaces adjusted patients’ work hours according to their treatment schedules, assigned work tasks as needed, and supported patients in taking a leave of absence for treatment.
Workplace allowances/systems needed to help patients continue working while undergoing treatment respondents emphasized the use of leave and paid leave systems, as well as general workplace flexibility and support.
Family support
Patients mentioned transportation and pick-up support to and from the hospital provided by family members, daily support during recuperation, emotional support, and medically related support.
Drafting a trial version of the information-gathering tool
RT sheet: The RT and BI questionnaires were developed based on previous literature and the opinions of the collaborators’ clinical experience. Items that required modification as treatment progressed were deleted, resulting in a final total of 13 items.
Relationships among BI sheet variables
Spearman’s rank correlation coefficient was calculated to examine the similarity of items. This analysis explored associations between key variables and determined their 95% confidence intervals. (Table 6) presents the results for items with strong and significant correlations, based on all Spearman’s rank correlation coefficients and their 95% confidence intervals. Five items showed further associations, allowing for cross-analysis and identification of significant differences:
Gender and whether or not one has a relative with cancer (χ²=4.381, df=1, p=0.036); gender and having private health in surance (χ²=6.873, df=1, p=0.009); having a relative with cancer and mode of transportation to hospital (χ²=7.467, df=1, p=0.006); use of healthcare benefits and knowing a patient (χ²=4.2, df=1, p=0.04); mode of transportation to hospital and experiencing symptoms (χ²=9.545, df=2, p=0.008).
Table 1: Survey study I.
| ID |
Age |
Sex |
Disease(clinical diagnosis) |
Treatment purpose |
Irradiationmethod |
Total dose (Gy) |
Treatment period (days) |
Irradiation area |
Presence of combined treatment |
If combinedtherapy, specific method |
Presence ofpretreatment beforetreatment |
Presence of bolus, shell |
| 1-2 |
48 |
2 |
Breast cancer |
Semi-definitive |
External beam radiation |
50 |
25 |
Chest |
Combination |
Hormone |
N/A |
Nothing |
| 1-3 |
68 |
1 |
Prostate cancer |
Semi-definitive |
IMRT |
74 |
37 |
Abdomen and pelvis |
Combination |
Hormone |
Yes |
Nothing |
| 1-4 |
51 |
1 |
Parotid cancer |
Semi-definitive |
IMRT |
66.03 |
34 |
Neck |
Nothing |
- |
N/A |
Yes |
| 1-5 |
66 |
1 |
Prostate cancer |
Semi-definitive |
External beam radiation, IMRT |
74 |
37 |
Abdomen and pelvis |
Combination |
Harmone |
Yes |
Nothing |
| 1-6 |
69 |
1 |
Prostate cancer |
Semi-definitive |
Other |
74 |
37 |
Abdomen and pelvis |
Combination |
Hormone |
Yes |
Nothing |
| 1-7 |
65 |
1 |
Prostate cancer |
Definitive |
IMRT, Other |
74 |
37 |
Abdomen and pelvis |
Combination |
Hormone |
Yes |
N/A |
Table 2: Survey study II.
| ID |
Age |
Sex |
Disease(clinical diagnosis) |
Treatment purpose |
Irradiationmethod |
Total dose (Gy) |
Treatment period (days) |
Irradiation area |
Presence of combined treatment |
If combinedtherapy, specific method |
Presence ofpretreatment beforetreatment |
Presence of bolus, shell |
| 2-1 |
65 |
2 |
Breast cancer |
Semi-definitive |
External beam radiation |
50 |
25 |
Chest |
Nothing |
|
Nothing |
Nothing |
| 2-2 |
66 |
1 |
Eye tumor |
N/A |
N/A |
N/A |
N/A |
Face |
Nothing |
|
Nothing |
N/A |
| 2-3 |
58 |
1 |
Laryngeal cancer |
N/A |
N/A |
N/A |
49 |
Neck |
Nothing |
|
N/A |
N/A |
| 2-4 |
63 |
2 |
Rectal cancer |
N/A |
External beam radiation |
60 |
30 |
Abdomen and pelvis |
Nothing |
|
Nothing |
Nothing |
| 2-5 |
63 |
1 |
Prostate cancer |
Definitive |
IMRT |
60 |
33 |
Abdomen and pelvis |
Combination |
Hormone |
Yes |
Nothing |
| 2-6 |
63 |
1 |
Prostate cancer |
N/A |
IMRT |
78 |
39 |
Abdomen and pelvis |
Nothing |
|
Nothing |
Nothing |
| 2-7 |
58 |
2 |
Breast cancer |
Semi-definitive |
External beam radiation |
60 |
30 |
Chest |
Nothing |
|
Nothing |
Nothing |
| 3-1 |
59 |
2 |
Breast cancer |
Semi-definitive |
External beam radiation |
50 |
25 |
Chest |
Nothing |
- |
Nothing |
Nothing |
| 3-2 |
57 |
2 |
Breast cancer |
Semi-definitive |
N/A |
N/A |
25 |
Chest |
Nothing |
- |
N/A |
N/A |
| 3-3 |
39 |
2 |
Breast cancer |
Semi-definitive |
N/A |
N/A |
26 |
Chest |
Nothing |
- |
N/A |
N/A |
| 3-4 |
60 |
2 |
Breast cancer |
Semi-definitive |
External beam radiation |
38 |
25 |
Chest |
Nothing |
- |
Nothing |
Nothing |
| 3-5 |
24 |
1 |
Colorectal cancer |
N/A |
N/A |
N/A |
N/A |
Abdomen and pelvis Chest |
N/A |
N/A |
N/A |
N/A |
| 3-6 |
54 |
2 |
lymphoma |
N/A |
N/A |
N/A |
N/A |
Groin |
Nothing |
- |
Nothing |
Nothing |
| 3-7 |
68 |
2 |
Breast cancer |
Semi-definitive |
N/A |
N/A |
N/A |
Chest |
Nothing |
- |
Nothing |
Nothing |
Table 3: Patient basic information and social factors information sheet (BI sheet).
| Items |
Survey studyn = 14 |
| Age |
Mean±SD |
56.93±11.8 |
| Gender |
Male |
5 |
| Female |
9 |
| Family structure |
1) Livingalone |
4 |
| 2) Coupleonly |
1 |
| 3) Livingwith children |
3 |
| 4) Livingwith parents |
2 |
| 5) Livingwith other relatives |
0 |
| 6) Livingwith non-relatives |
1 |
| 7) Other |
1 |
| N/A |
2 |
| Highest education level |
1) Compulsory education |
0 |
| 2) Highschool |
6 |
| 3) Vocational school |
3 |
| 4) University |
3 |
| 5) University master’s degree |
1 |
| 6) Graduate school doctoral degree |
0 |
| 7) Juniorcollege |
1 |
| Profession |
1) Managerial worker |
1 |
| 2) Professional/technical worker |
8 |
| 3) Officeworker |
2 |
| 4) Salespersonnel (real estateindustry, pharmaceutical sales,etc.) |
0 |
| 5) Service worker (domestic help,care staff, etc.) |
1 |
| 6) Security worker (police officer, coast guard, etc.) |
0 |
| 7) Agriculture, forestry, and fisheyworker |
0 |
| 8) Production process worker |
0 |
| 9) Transportation/machine operating personnel |
0 |
| 10) Construction/mining worker |
1 |
| 11) Other |
1 |
| Job position |
1) Generalstaff |
7 |
| 2) Sectionchief/section manager, etc. |
1 |
| 3) Deputymanager/department chief |
1 |
| 4) Chairman, president, managing director, etc. |
0 |
| 5) Other( ) |
5 |
| Income |
1) <3million yen |
6 |
| 2) 3.01million yen to 5 millionyen |
6 |
| 3) 5.01million yen to 8 millionyen |
1 |
| 4) 8.01million yen to 10 millionyen |
0 |
| 5) ≥10,010,000 yen |
1 |
| Height |
Mean ± SD |
162.8 ± 9.12 |
| Body weight |
Mean ± SD |
62.22 ± 7.01 |
| Presence of weight gain/loss |
1) Yes → Pleaseproceed to question 10 |
6 |
| 2) No → Pleaseproceed to question 11 |
8 |
| Medical history |
Free textresponse |
|
| Presence or absence of dental carecover |
1) Yes |
10 |
| 2) No |
2 |
| N/A |
2 |
| Presence or absence of cancer screening |
1) Attended every year withoutfail |
1 |
| 2) Attended only at the target age |
5 |
| 3) Almostnever attended |
7 |
| 4) Other( ) |
1 |
| Has a relative withcancer |
1) Yes → Pleaseproceed to question 10 |
8 |
| 2) No → Pleaseproceed to question 11 |
6 |
| Type of relative with cancer |
1) Firstdegree relative (parent, child) |
6 |
| 2) Seconddegree relative (grandparent, grandchild, sibling, etc.) |
0 |
| 3) Other( ) |
2 |
| Smoking status/years of smoking |
1) Neversmoked |
6 |
| 2) Previous smoking history (smoked for years) |
6 |
| 3) Currently smokes (smoked for years) |
2 |
| 4) Other( ) |
0 |
| Alcohol consumption |
1) Doesnot or cannotdrink alcohol |
6 |
| 2) Occasional drinker |
3 |
| 3) Drinksalcohol every day |
4 |
| 4) Other( ) |
0 |
| N/A |
1 |
| Do you thinkthat once you have madea decision, you would carryit out even if it took a long time,regardless of the type of decision? |
1) Yes |
8 |
| 2) No |
6 |
| What aspectsof your dailylife make you feel like you're makingan effort? |
Free textresponse |
|
| Who was the firstperson you toldwhen you foundout you weresick? |
Free textresponse |
|
| Have you everconsulted with a medical professional other than yourprimary care physician? |
1) Yes |
4 |
| 2) No |
10 |
| Is there anyonewho has had a positive impact on your receiving radiation therapy? |
1) Yes |
10 |
| 2) No |
4 |
| What systemdid you useto attend treatment? |
1) Paidvacation system (usedon a daily basis) |
4 |
| 2) Paidvacation system (usedin half-day units) |
1 |
| 3) Paidvacation system (usedon an hourlybasis) |
1 |
| 4) Used the company's unique leave/vacation system |
1 |
| 5) Injuryand Sickness Allowance |
1 |
| |
6) High-cost medical treatment system |
4 |
| 7) Other( ) |
1 |
| N/A |
1 |
| Did your workplace makeallowances for you during treatment |
1) Yes |
13 |
| 2) No |
1 |
| Are there allowances and systems you think yourworkplace should havein place to help youcontinue your workand treatment? |
1) Yes |
8 |
| 2) No |
1 |
| 3) I can’t thinkof anything specific |
4 |
| N/A |
1 |
| Free textresponse |
|
| Are you awareof the existence of patient associations and family associations? |
1) Yes |
5 |
| 2) No |
9 |
| Do you want information about patient andfamily groups? |
1) Yes |
0 |
| 2) No |
11 |
| N/A |
3 |
| Have you everreceived support froma patient association or family association? |
1) Yes |
2 |
| 2) No |
4 |
| N/A |
8 |
| Have youever received supportfrom your family? |
1) Yes |
6 |
| 2) No |
7 |
| N/A |
1 |
| Have you everreceived support froma healthcare professional in an outpatient setting? |
1) Yes |
4 |
| 2) No |
9 |
| N/A |
1 |
| Is there any support you would likefrom a healthcare professional so youcan continue to work and receive treatment? |
1) Yes |
4 |
| 2) No |
2 |
| 3) I can’t thinkof anything specific |
6 |
| N/A |
2 |
| Are you doing anything else other than attending treatment? |
1) Yes |
7 |
| 2) No |
3 |
| N/A |
4 |
| Time takento visit thehospital |
Mean ± SD |
40.18 ± 33.67(minutes) |
| Duration of hospital visit |
Mean ± SD |
50.71 ± 22.69(minutes) |
| Main transportation method used to attend hospital in the lastweek |
1) Publictransport |
3 |
| 2) Taxi |
0 |
| 3) Walking |
0 |
| 4) Privatecar (driven by yourself) |
10 |
| 5) Privatecar (driven by family) |
1 |
| 6) Other |
0 |
| Have private insurance |
1) Yes ⇒ Please proceed to question 46 |
11 |
| 2) No ⇒This survey has ended |
3 |
| Type of insurance |
1) Medicalinsurance (covers a wide rangeof illnesses andinjuries) |
9 |
| |
2) Cancerinsurance (covers cancer) |
1 |
| 3) Specific healthcare insurance for three majorillnesses (cancer, acutemyocardial infarction, and stroke) |
1 |
| 4) Other( ) |
0 |
| What prompted you to enrollin this insurance policy? |
Free textresponse |
|
Table 4: Categorization of interview research.
| Categories |
Subcategories |
Code |
| Decision makingprocess |
Source of information collection |
Family, relatives |
| people at work |
| Patient and family meetings |
| Internet (SNS,blogs, etc.) |
| Influence on decision making |
Opinions of medical professionals |
| Stories from people who have experienced the same illness |
| Experience duringtreatment |
Experience of balancing treatment and work |
Advantages anddifficulties of balancing both |
| How to deal with difficulties |
| What we are tryingto do |
| Adjustment of treatment schedule |
Inconvenient treatment time |
| Treatment flexibility needs |
| Support and resources |
Support from the workplace |
Taking vacation |
| Adjustment of working hours |
| Understanding and cooperation in the workplace |
| Systems used (e.g. high-cost medical system, paidholidays, etc.) |
| support fromfamily |
emotional support |
| Physical support(e.g. transportation, visits, medical treatment, etc.) |
| Information andsupport network |
Patient and family meetings |
knowledge and interest |
| Support received |
| Effectiveness of information sources |
Usefulness as a sourceof information |
| How to access information |
Table 5: Free-form responses to the questionnaire.
| Making an effortin daily life |
| Category |
Code |
| Eating habits |
Avoiding processed foods and instantnoodles# |
| Eating properly |
| Changing the order of meals (ricelast) |
| Movement |
Walking home(1 hour) |
| Exercising (badminton) |
| Dedication to workDedication to work |
Going to work withoutsufficient rest |
| Going to work and cleaning earlier than others |
| Getting up earlier thanusual and continuing with current treatment |
| Doing my best as the executive committee chairperson for the summerfestival at work |
| |
Not speaking ill of others(complaining) # |
| Consideration for family |
Balancing workwith caring for my biological mother who liveswith me and my fatherwho is hospitalized# |
| Time management and efficiency |
Trying to avoid wasting time as muchas possible |
| Doing everything efficiently and withoutmaking mistakes |
| Nothing special |
Nothing in particular |
| Allowances made by the workplace during treatment |
| Category |
Code |
| Adjustment of working hours |
Change to working times |
| Reduction in working hoursby 30 minutes |
| Being lateowing to treatment |
| Paid leaveand working hours# |
| Allowed to go home after treatment # |
| Business coordination/support |
Work coveredby other staff# |
| I am asked to share the work I am responsible for # |
| Allowances regarding leaveof absence |
I havean unlimited leaveof absence, and my healthis a priority for me # |
| I was able to rest # |
| Injury and sickness benefits are available whileI am on leave # |
| Special considerations for treatment |
Although I work in Kyoto, I received treatment in Nagasaki for 33 days |
| Other considerations |
Freedom to go to work |
| No specific instructions for treatment |
| Workplace allowances/systems neededto help patients continue working whileundergoing treatment |
| Category |
Code |
| Use of vacations andpaid systems |
Paid vacation system, no holidays, but you can take sickleave (this can also takethe form of absenteeism) # |
| It wouldbe nice to be paidby the hour |
| You feelfree to takepaid leave or days off in half-day or hourly increments |
| Flexibility in theworkplace Flexibility in the workplace |
Allowances for treatment time |
| To avoidinconvenience at work,I ask the hospital for treatment firstthing in the morning to reduce the burden |
| I would likemy workplace to either not divulge thereason for my taking time to the rest of the staffor to provide an appropriate alternative explanation |
| I'm thinking about changing departments # |
| Allowance for treatment time |
| Workplace socialsupport |
A work environment whereyou can obtainunderstanding and cooperation from colleagues # |
| I wantto come back to workafter my courseof treatment # |
| Family support |
| Category |
Code |
| Transportation |
Drop-off andpick-up when visiting the hospital # |
| Transportation to and fromhospital # |
| Transfer |
| Daily livingsupport during medicaltreatment |
It's comingsoon # |
| Taking careof meals etc. during medicaltreatment # |
| Did the housework by themselves |
| Provided whatI needed |
| Emotional support |
Spiritual follow-up # |
| Calling me |
| Medical support |
Meetings beforeand after surgical operation, meeting with the attending physician # |
| Accompanying my mother who lives withme to the hospital # |
| Helping my hospitalized fatherwith hospital transfers # |
| Engagement in activities other than treatment |
| Category |
Code |
| Diet and nutrition |
Contents of meals # |
| Physical activity and exercise |
Exercises you can do at home# |
| Exercises such as walking |
| Movement |
| Stretching # |
| Easy stretches |
| Walking the dog # |
| I go outside as much as possible # |
| Relaxation and rest |
Taking a relaxing holiday |
| Taking a leisurely bath |
| Ideas for daily life |
Choosing the timing of a bath(taking a bath in the evening to keep my body cool)# |
| Health monitoring |
Self-management by measuring body temperature, weight,and blood pressure # |
| Nothing in particular/none |
Nothing in particular |
# Interview data.
Table 6: Spearman correlation coefficient between 36 items and 95% confidence interval (two-tailed).
| |
Spearman correlation coefficient |
p-value |
95% confidence interval(two-tailed) |
X2 test |
p-value |
df |
| lower limit, |
upper limit |
|
| Gender -Disease |
-0.692 |
0.006 |
-0.898 |
-0.239 |
/ |
|
|
| Gender-combined |
-0.546 |
0.043 |
-0.84 |
-0.004 |
ns |
|
|
| Gender-Checkup |
-0.669 |
0.009 |
-0.889 |
-0.197 |
ns |
|
|
| Gender- Cancerin a relative |
-0.559 |
0.038 |
-0.846 |
-0.024 |
4.381 |
0.036 |
1 |
| Gender- Insurance |
-0.701 |
0.005 |
-0.901 |
-0.254 |
6.873 |
0.009 |
1 |
| Disease-Checkup |
0.785 |
<.001 |
0.422 |
0.931 |
/ |
|
|
| Irradiation area- weight gain/loss |
-0.6 |
0.023 |
-0.862 |
-0.085 |
/ |
|
|
| Irradiation area-drinking |
-0.564 |
0.036 |
-0.847 |
-0.03 |
/ |
|
|
| Irradiation area- system available |
0.575 |
0.031 |
0.047 |
0.852 |
/ |
|
|
| Combined use - Who did youtell? |
0.571 |
0.033 |
0.04 |
0.85 |
/ |
|
|
| Family type - paidper day |
0.545 |
0.044 |
0.003 |
0.84 |
/ |
|
|
| Educational background-Position |
0.615 |
0.019 |
0.108 |
0.868 |
/ |
|
|
| Weight gain/loss-drinking |
0.606 |
0.021 |
0.095 |
0.865 |
/ |
|
|
| Medical history- who did you tellit to? |
0.567 |
0.034 |
0.035 |
0.849 |
/ |
|
|
| Past medicalhistory - usedthe system |
0.57 |
0.033 |
0.04 |
0.85 |
/ |
|
|
| Medical check-up - hourly paid |
-0.555 |
0.039 |
-0.844 |
-0.017 |
/ |
|
|
| Medical examination-injury and disease |
-0.555 |
0.039 |
-0.844 |
-0.017 |
/ |
|
|
| Cancer in a relative - Means of going to the hospital |
-0.73 |
0.003 |
-0.912 |
-0.31 |
/ |
|
|
| Cancer in a Relative - Current Symptoms |
0.599 |
0.024 |
0.083 |
0.862 |
/ |
|
|
| Smoking - Who did you tell? |
0.593 |
0.026 |
0.073 |
0.859 |
/ |
|
|
| Smoking - Support fromfamily |
0.546 |
0.044 |
0.004 |
0.84 |
/ |
|
|
| Who did you tell- support from your family |
0.601 |
0.023 |
0.086 |
0.862 |
/ |
|
|
| Other thanthe attending physician - Today's PS |
-0.558 |
0.038 |
-0.845 |
-0.022 |
7.467 |
0.006 |
1 |
| There is a systemavailable - one day paid |
0.683 |
0.007 |
0.223 |
0.894 |
ns |
|
|
| Injury and illness - patient association |
-0.548 |
0.043 |
-0.841 |
-0.007 |
/ |
|
|
| Injury andillness - Outpatient support from medical professionals |
-0.599 |
0.024 |
-0.862 |
-0.083 |
/ |
|
|
| Patient Association - Today's PS |
-0.611 |
0.02 |
-0.866 |
-0.101 |
/ |
|
|
| Support fromfamily - rest |
0.555 |
0.039 |
0.017 |
0.844 |
ns |
|
|
| Support fromfamily - Sleep |
0.555 |
0.039 |
0.017 |
0.844 |
14 |
0.001 |
2 |
| Means of visiting hospital -Current symptoms |
-0.82 |
<.001 |
-0.943 |
-0.5 |
4.2 |
0.04 |
1 |
When an appropriate test cannot be performed, a slash (/) is inserted in the table. If no significant difference is observed, 'ns' (not significant) is indicated.
Discussion
Selection of survey targets
The Japanese prefectures where University Hospital A and University Hospital B are located both have numerous islands. The sample size was set at 14, which was considered sufficient to reach data saturation in the qualitative analysis. It was anticipated that some participants might struggle to balance treatment and work, potentially leading to leave of absence or hospitalization. Perhaps for this reason, Hospital A devised a way to complete the radiotherapy treatment. However, the results indicate that local municipalities, including those on islands, need to ensure patients’ access to medical facilities. Therefore, it should be recognized that the means of attending hospital visits and the patient’s place of residence are important information during the treatment planning stage.
Analysis of BI questionnaire responses
Exploration of the relationship between variables on the BI sheet: The results of the quantitative data analysis suggest that gender strongly interacts with these factors. In Japanese literature, site-specific studies on radiotherapy have focused on head and neck, breast, prostate, and pelvic cavity diseases [4], indicating that gender significantly influences these factors. Additionally, the findings suggest that gender affects whether radiation therapy and concomitant treatments are used. For example, prostate cancer patients often continue to experience side effects from hormone therapy post-treatment, including physical functioning issues that impact their psychological well-being [4]. This implies that gender and the presence or absence of concomitant treatments both play significant roles in patient outcomes.
The χ² test with cross-tabulation identified significant associations between gender and having a relative with cancer, and between gender and private health insurance status. Further studies are warranted to explore how these variables affect patients’ health behavior and risk perception. Additionally, significant differences were found between the means of transportation to the hospital and the presence of symptoms, suggesting that transportation is chosen according to the presence of symptoms and that the convenience of transportation to the hospital may affect patients’ perception of symptoms.
Furthermore, regarding the socioeconomic effects of education, job position, and family type, a significant positive correlation was found between education and job position, with more educated individuals having higher job positions.
The validity of the questionnaire items was examined in terms of (1) content validity, (2) clarity of expression, (3) ease of response, and (4) logical sequence. As a result, some questions were combined, and expressions were revised to ensure clarity and reduce complexity.
Results of qualitative analysis
Summary of free responses on the survey BI sheet: The free-response statements from the five respondents on leave and the nine respondents still working could not be categorized and analyzed separately because of the small sample size. Therefore, all responses were analyzed collectively and categorized into five themes.
Lifestyle improvement activities beyond treatment: Patients engaged in various lifestyle improvement activities outside of treatment to maintain their health. A previous study [5] indicated that outpatient cancer patients expect outpatient nurses to acknowledge their lifestyle changes and efforts, emphasizing the importance of the knowledge and attitudes of nurses. Patients’ efforts should be recognized, and nurse-patient dialogue should be emphasized. And for self-management to be effective, cancer patients and survivors must be supported in managing their symptoms and conditions [7].
Effort and dedication
With the improvement in cancer survival rates and advancements in treatment, many cancer patients continue to work while undergoing treatment. It is estimated that approximately 499,000 people attend hospitals for cancer treatment while remaining in employment [8]. According to Japanese Ministry of Health, Labour and Welfare guidelines, flexibility is required during treatment, and employers should respond flexibly to changes in workers’ physical conditions [8]. Hence, the use of information-gathering tools to assess the individual situations of employees is essential. In a study aimed at identifying the efficacy of an ANI in promoting a balance between treatment and the social roles of cancer patients receiving outpatient chemotherapy and radiation therapy [9], the algorithm was centered on building relationships, increasing the balance between mind and body, and personalized coordination of nursing roles to maintain patients’ social roles, including employment, to relieve cancer patients’ pain and nurture their strengths [9].
Allowances in the workplace
A previous study on balancing treatment and work for cancer patients [10] concluded that organizational nursing professionals implemented support through “collaboration and coordination,” “environmental improvements,” and “privacy considerations.” Nursing professionals need to fully examine and respond to individual cases both in workplaces and hospitals. There is an increasing need for information-gathering tools to clarify individual situations.
Support from families
The Basic Plan for the Promotion of Cancer Control [11], an initiative by the Japanese government, prioritizes “cancer control for the working generation,” and addresses the employment needs and issues of cancer patients and their families. However, it lacks sufficient mention of family support. It is clear that family support for hospital visits and daily life activities contributes to the psychological well-being of patients. Employment support for cancer patients should encompass family support.
Summary of interview data
Four categories were identified from the qualitative analysis of the interview data.
Decision-making process
Patients gathered information and exchanged opinions with family members, colleagues, patient associations, and online platforms when making treatment choices. Professional support is needed to help cancer patients make appropriate decisions. Although the establishment of cancer consultation support centers based on the general hospital system for cancer treatment [12] has improved decision-making support, and the use of these centers has increased, further specialized support is needed.
Experiences during treatment
Balancing treatment and work was a major challenge for many patients, and patients often found it difficult to coordinate work hours and treatment schedules. The patient interview narratives indicated that inadequate support in the workplace led to emotional stress. Japanese governmental guidelines suggest that, in addition to provision of leave, employers need measures that take into account workers’ health status and work ability according to their disease symptoms, treatment side effects, and disabilities [13]. It is important to promote understanding within the workplace and foster cooperation among coworkers.
Support and resources
Although systems such as paid leave and sickness benefits were available, the level of support varied across workplaces. Nursing professionals in organizations need to collaborate with other departments as knowledgeable advocates for patients’ disease status and characteristics, and implement practices to improve the work environment for cancer patients [5]. The Japan Organization of Occupational Health and Safety “Manual for Supporting Workers with Cancer to Balance Treatment and Employment” [14] suggests the need for medical professionals to provide employment support for cancer patients.
Information and support networks
Although patient and family associations are recognized by the participants of this study, they are not fully utilized. A previous study showed that outpatient nurses provided five types of social support to patients (emotional, informational, instrumental, evaluative, and predictive support) with the aim of identifying the most suitable type of support for each patient to help them continue treatment and improve their quality of life [15]. It is important to identify and use the most appropriate type of support for each patient. For example, in the context of Immunotherapy (IO), patients often obtain treatment information through online communities. That report stated that «12 participants joined online communities, including Facebook and Google Groups, where they could pose questions and solicit advice from others treated with IO [15,16]».
Draft a prototype of the “information gathering tool
RT sheet
The RT and BI sheets were originally created by reviewing previous studies [4,5] and relevant literature. For instance, the latest Ethos treatment system for cancer radiation therapy (Varian Medical Systems) uses AI-driven automatic contouring and planning optimization to adapt radiation delivery to anatomical changes, potentially improving treatment accuracy [6]. This device modifies the number of treatments per day and the dose per session (in gray) as treatment progresses by optimizing tumor contouring and planning. Thus, as found in the study referenced in citation [6], cancer radiation therapy adapted the irradiation to anatomical changes in the tumor, which resulted in the elimination of unnecessary data. Consequently, the number of items was reduced to 14. 2) BI Sheet.
The content validity of the BI sheet was reviewed by the coresearchers. This led to the deletion of 14 items from the original 47-item scale, leaving 33 items. The conceptual relevance of each item was evaluated and the entire scale refined.
Evaluation of the SP sheet
The SP sheet comprises six items and was used to assess daily changes in variables before the start of treatment and as treatment progressed.
Potential use of the tool
This information-gathering tool could help to assess the physical and psychological reactions of patients undergoing cancer radiation therapy and the social effects of treatment. This would permit the early identification and resolution of problems. As new or inexperienced nurses may struggle to provide effective emotional support to patients [17,18], this tool was designed to be user-friendly and to help patients balance treatment and work. It could be used to identify factors that enable patients to continue outpatient radiation therapy, enhance patient understanding of potential issues, and facilitate timely interventions.
Conclusion
The following conclusions can be drawn from the study findings.
Geographical considerations: Island hospitals are affected by geographical characteristics, emphasizing the importance of considering patients’ modes of transport and places of residence. This suggests the need for a unique regional approach to ensure that patients complete radiotherapy.
Gender-specific care: Gender substantially affects healthcare-related variables such as the choice of radiation therapy and combination therapy, cancer screening uptake, and family history. This underscores the need for care tailored to the needs of female patients.
Socioeconomic factors: Patients’ socioeconomic backgrounds affect access to treatment and workplace support. Higher education and job positions, along with family status, affect paid employment, necessitating a comprehensive support program that considers these factors.
Work and treatment balance: Effective support to help patients balance treatment and work involves issues of schedule adjustments and workplace absences/pensions. Flexibility in treatment scheduling is important.
Family support: Family support, including transportation, daily life assistance, and emotional follow-up, is essential for patients undergoing treatment. These factors contribute substantially to maintaining patients’ quality of life.
Development of new tools: This study highlights the need for new information-gathering tools for detailed assessment of the physical and psychological reactions and social influences of patients undergoing radiotherapy, to help them to balance treatment and work.
These findings could contribute to a comprehensive understanding of the diverse challenges faced by patients undergoing radiotherapy and the development of effective countermeasures that provide a basis for improved patient support and quality of care.
Limitations of the study
In this study, we developed a prototype draft of an information-gathering tool and surveyed 14 participants as part of a mixed-methods exploratory study. Although a pilot test was needed to examine the reliability and validity of this original scale, such a test could not be conducted owing to the effects of Covid-19. Additionally, because of various social changes in Japan, such as work reforms, we were limited to collecting qualitative and exploratory quantitative data at this prototype stage.
Therefore, there is a need for a larger-scale quantitative survey using the developed tool to obtain results that can be generalized to a larger population of cancer patients. Such a survey should be performed in one or two phases to confirm the reliability and validity of the tool. Furthermore, a study should be conducted to examine the validity of this information-gathering tool against the Japanese version of the Quality of Life Radiation Therapy Instrument for radiation therapy patients, which was developed by the Japanese Society for Therapeutic Radiology and Oncology Quality of Life Evaluation Study Group [18]. Additionally, we plan to incorporate the views of researchers from other disciplines, along with our collaborators, when reviewing this tool to identify factors that may affect the interpretation of the results.
Declarations
Acknowledgment: We would like to express our sincere gratitude to the nurses of the medical institutions who were the participants of this study, and to the nursing directors and chief nurses of the medical institutions who cooperated with us in conducting this study. We thank Diane Williams, PhD, from Edanz (https://jp.edanz.com/ac) for editing a draft of this manuscript.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Acknowledgments: We thank all the participants and staff involved in this study for their contributions and support.
Credit author statement: The authors collectively contributed to the conception and design of the study. Data collection was undertaken by Yumiko Kanamaru, who also led the data analysis with support from Tamami Koyama, Yumiko Tsuchhashi, and Yuko Matsunari. All authors were granted complete access to all the data in the study, with the corresponding author bearing the final responsibility for the decision to submit for publication. The corresponding author affirms that all listed authors fulfill the authorship criteria and that no others meeting the criteria have been omitted.
Conflicts of interest: All authors have no conflicts of interest to declare.
Funding: This research was funded by JSPS KAKENHI grant numbers 18K17487.
Ethics statement: The research was approved by the ethics review committee of Kagoshima University’s School of Medicine and Dental Hospital (Reception No.: 170136 Epidemic-Revision 2). The research was approved by the ethics review committee of Nagasaki University Hospital (Reception No.: 18052116 Epidemic-Revision 2). Informed consent was obtained from all individual participants included in the study.
Data availability statement: The datasets generated and/or analyzed during the current study are not publicly available due to privacy and confidentiality commitments made to the participants at the time of data collection. The data are securely stored in a locked archive, accessible only to the research team. Data access requests can be directed to the corresponding author and will be considered on a case-by-case basis, subject to necessary ethical approvals and agreements to maintain the confidentiality of the data.
Declaration of generative AI and AI-assisted technologies in the writing process: No AI tools/services were used during the preparation of this work.
References
- Takashi Uno. Welcome from the President of JASTRO 2024. https://www.jastro.or.jp/en/about_jastro/welcome_from_the_president.html
- Van de Schoot AJ, Hoffmans D, Van Ingen KM, et al. Characterization of Ethos therapy systems for adaptive radiation therapy: A multi-machine comparison. Journal of Applied Clinical Medical Physics. 2023; 24: e13905. https://doi.org/10.1002/acm2.13905.
- Kato T, Kikuno N, Hata K, et al. Radiation Therapy Notebook for application of patient-centered radiation practice. The Journal of Radiological Nursing Society of Japan. 2023; 11: 42-52. https://doi.org/10.24680/rnsj.RJ-12003.
- Kanamaru Y, Matsunari Y, Tsuchihashi Y. Current status and issues of nursing care research in radiotherapy: examination of domestic documents and overseas documents. Bulletin of the School of Health Sciences. Faculty of Medicine, Kagoshima University. 2017; 27: 29-38.
- Tamami K, Takumi Y, Yumiko K, et al. The contents of balancing support for cancer patients between treatment and employment and that of difficulties, by nurses: A literature review. Bulletin of the School of Health Sciences. Faculty of Medicine, Kagoshima University. 2022; 32: 21-28.
- Benner P. From novice to expert. American Journal of Nursing.1986; 82: 402-407.
- Rebekah Park, James W Shaw, Alix Korn, Jacob Mc Auliffe. The value of immunotherapy for survivors of stage IV non-small cell lung cancer: Patient perspectives on quality of life. Journal of Cancer Survivorship. 2020; 14: 363-376.
- Ministry of Health, Labour and Welfare. Guidelines for supporting the balance between treatment and occupational life in workplaces. 2016.https://www.mhlw.go.jp/content/11200000/000621298.pdf.
- Kanda K, Kyota A, Fujimoto K, et al. Efficacy of an Algorithm-Based Nursing Intervention to Promote a Balance Between Cancer Patients’ Social Roles and Outpatient Treatment. A Quasi-Experimental Study. Cancer Nursing. 2023; 46(4): 303-313.
- Hashimoto R, Imai Y. Working situations of patients with cancer: A literature review. The Journal of Nursing Investigation. 2019; 17: 1-9.
- Ministry of Health, Labour and Welfare. Basic plan for cancer control promotion. 2012. https://www.mhlw.go.jp/bunya/kenkou/dl/kenkounippon21_02.pdf.
- Ministry of Health, Labour and Welfare. Consultation support at base hospitals for cancer treatment. https://www.mhlw.go.jp/file/05-Shingikai-10901000-Kenkoukyoku-Soumuka/0000186422.pdf
- Ministry of Health, Labour and Welfare. Guidelines for supporting the balance between treatment and occupational life in workplaces. 2024. https://www.mhlw.go.jp/content/11200000/001225327.pdf
- Japan Organization of Occupational Health and Safety. Manual for supporting workers with cancer to balance treatment and work. 2017. https://www.johas.go.jp/Portals/0/data0/kinrosyashien/pdf/bwt-manual_cancer.pdf
- Tamura M, Suetsugu N, Sukehiro A. Literature review about social support for cancer patients: for support to patients at outpatient department. The South Kyusyu Journal of Nursing. 2013; 3(11): 37-45.
- Oluwaseyifunmi Andi Agbejule, Nicolas H Hart, Stuart Ekberg, Raymond Javan Chan. Development of a self-management support practice framework for addressing cancer-related fatigue: a modified Delphi study. Journal of Cancer Survivorship. 2024; 18: 972-982.
- Tsuchihashi Y, Matsunari Y, Kanamaru Y. Survey of difficult experiences of nurses caring for patients undergoing radiation therapy: an analysis of factors in difficult cases. Asia Pac J Oncol Nurs. 2018; 5(1): 91-98. https://doi.org/10.4103/apjon.apjon_48_17
- Karasawa K, Sasaki T, Okawa T, et al. Development of QOL-RTI Japanese Version (General And Head & Neck Module)- Results of a clinical trial and revision Final Version-Journal of the Japanese Society for Therapeutic Radiology and Oncology. 2002; 13: 185-193.