Introduction
Breast Cancer (BC) is the most common malignant tumor [1] in women in our country, and breast lymphoma is a rare malignant tumor that can be divided into primary and secondary types according to the tissue type of origin. The incidence of Breast Lymphoma (BL) ranges from 0.04% to 0.7% [2], and its low incidence may be related to the lack of lymphatic tissue in the breast. BL includes PBL and SBL. The imaging features of both are nonspecific, and the imaging phenotypes of the two tumors overlap with those of other breast malignancies, making diagnosis challenging PBL is a rare type of Non Hodgkin Lymphoma (NHL), which accounts for 0.04%-1.00% of breast malignancies and only 1.7%-3.0% [3-5] of all NHL. Diffuse Large B Cell Lymphoma (DLBCL) is the most common pathological type, accounting for 56% to 84% [6]. More than 98% of patients with Primary Breast Diffuse Large B Cell Lymphoma (PB-DLBCL) are female [7]. The clinical manifestation of PB-DLBCL is lack of opposite-sex, clinical diagnosis is difficult, and its malignancy degree is high, rapid progression, 5-year survival rate is 20%-76% [8,9]. Due to the low incidence of BL and the lack of large-scale clinical trials to explore the results, there is no consensus on the best treatment plan for BL. The common treatment method is anthracycline-containing chemotherapy combined with radiotherapy [10]. At first diagnosis, BL is often difficult to distinguish from breast cancer, and is often misdiagnosed as breast cancer, and is treated according to conventional breast cancer diagnosis. This study included 16 newly treated patients diagnosed with BL in Liaoning Cancer Hospital from January 2014 to December 2022, and analyzed their clinical data to explore the related prognostic factors and reasonable treatment mode of BL, and provide clinical reference for the reasonable diagnosis and treatment of BL.
Data and methods
Clinical data
The clinical data of 16 patients with BL diagnosed in Liaoning Cancer Hospital from 2014 to 2022 were retrospectively analyzed. The diagnosis of lymphoma was made according to WHO classification criteria for hematopoietic and lymphoid tissue tumors in 2008. The diagnosis of PB-DLBCL is strictly based on the diagnostic criteria proposed by Wiseman and Liao [11] in 1972: (1) there are sufficient pathological diagnostic specimens with both lymphoma invasion and normal breast tissue; (2) no prior history of malignant lymphoma outside the mammary gland; (3) the breast is the primary site, simultaneous or secondary ipsilateral axillary lymph node metastasis (if the simultaneous lymph node volume is larger than the breast mass or the mass is located in the axillary tail, should be considered as nodular lymphoma); (4) Microscopically, lymphomatous cell infiltration in the lobules and ducts of the breast was observed, but there was no evidence of malignant transformation in the mammary gland epithelium. The clinical stages were judged according to Ann Arbor standards [12] and combined with physical examination, mammography, ultrasound, mammography, chest X-ray or CT, abdominal B-ultrasound or CT, bone marrow puncture and other examinations. The invasion of both mammary glands was IVE stage, and there was no stage III. Age, tumor size, clinical stage, immunohistochemical results, laboratory data, baseline Lactate Dehydrogenase (LDH) levels, white blood cell, LDH levels were evaluated for the 16 patients. The clinical data of the 16 patients were followed up and recorded, including age, laboratory data [WBC count], treatment status (surgery, chemotherapy, radiotherapy, and scabbard injection).
Evaluation of therapeutic effect
According to the evaluation criteria of lymphoma efficacy, Cheson and [13] other remission rates were divided into Complete Remission (CR), Partial Remission (PR), and stable disease remission (stable disease), respectively. SD, Progressive Disease (PD) and disease relapse.
Follow-up
All patients were followed up by telephone or outpatient visits until June 2023. Progression Free Survival (PFS) was defined as the time from initiation of treatment to disease progression/recurrence or the last follow-up. Overall Survival (OS) was defined as the time from diagnosis until the patient’s death or last follow-up.
Statistical treatment
SPSS 25.0 software was used for statistical analysis. Kaplan-Meier method was used to calculate the cumulative survival rate of patients, Log-rank test was used for inter-group comparison, univariate and multivariate analysis was performed by Cox proportional risk model. All variables with P< 0.05 in the univariate analysis were included in the multivariate analysis, and the Forward method based on partial maximum likelihood estimation (LR) was used for analysis. P<0.05 was considered statistically significant.
Results
Clinical features of patients
A total of 16 inpatients with BL were included in this study, all of whom were female, ranging in age from 30 to 79 years, with a median age of 64 years. Sixteen patients were included, including 6 patients with PBL and 10 patients with SBL. Of the 6 patients with PBL, 3 had mass diameters < 5 cm and 3 had mass diameters ≥5 cm. In SBL patients, due to the fact that breast mass enlargement was less obvious than that of PBL, the baseline LDH level was increased in 6 patients, and the WBC level in 16 patients was within the normal duty range. According to the Ann Arbor staging system, 1 patient has been the 3,320 stage, 4 have been stage II and 11 have been stage IV. All patients were further classified, 11 were DLBCL subtype and 2 were NK/TL type. 1 case was FL type, 1 case was PTCL type and 1 case was BCL type. Ki-67 immunohistochemical tests were performed in 10 of all cases, of which 4 were Ki67≤70% and 6 were Ki67>70%. The specific clinical case data were shown in (Table 1).
Treatment characteristics of patients
Eight patients received chemotherapy alone, 2 patients received chemotherapy combined with targeted therapy, 5 patients received chemotherapy sequential radiotherapy, and 7 patients received surgery. The surgical methods included simple lumpectomy, segmentectomy, radical surgery, and modified radical surgery. None of the patients with SBL had surgery to treat the breast mass locally. Three patients received the CHOP (Cyclophosphamide, Doxorubicin, Vincristine, Prednisone) regimen, seven patients received the RCHOP (Rituximab, Cyclophosphamide, Doxorubicin, Vincristine, Prednisone) regimen, and one patient received the RHyper-CVAD regimen A and regimen B for a median of 6 cycles of chemotherapy. One patient received stem cell transplantation during treatment, and one patient received cytarabine intrathecal injection during treatment. The specific treatment characteristics are shown in (Table 1).
Table 1: Clinical case data.
| Case Type |
genders |
age |
onsetposition |
Maximum diameter |
Surgery or not |
Clinical Stages |
follow-up period |
patdological diagnosis |
lactate dehydrogenase |
Treatment Programs |
| 1-PBL |
female |
79 |
Right |
2 cm |
Yes |
IV |
32 montds* |
BCL |
160 |
C+R |
| 2-PBL |
female |
46 |
Left |
5 cm |
No |
II |
8 montds* |
DLBCL |
Null |
C+R |
| 3-PBL |
female |
68 |
Left |
uncertain |
Yes |
IV |
18 montds* |
DLBCL |
Null |
C+R+T |
| 4-SBL |
female |
73 |
Right |
3 cm |
Yes |
II |
6 montds # |
DLBCL |
206 |
C+R |
| 5-SBL |
female |
46 |
Left |
3.5cm |
No |
IV |
Lost |
DLBCL |
363 |
C+S |
| 6-PBL |
female |
69 |
Left |
3 cm |
Yes |
IIIE stageA group |
82 montds* |
DLBCL |
188 |
C+R+T |
| 7-PBL |
female |
60 |
Left |
6 cm |
No |
II |
16 montds* |
NK/TL |
Null |
NO |
| 8-PBL |
female |
49 |
Right |
8 cm |
No |
IV |
38 montds * |
DLBCL |
181 |
C |
| 9-SBL |
female |
68 |
Left |
3.5cm |
Yes |
IV stage Agroup |
44 montds # |
NK/TL |
208 |
C+T |
| 10-SBL |
female |
30 |
Right |
uncertain |
No |
IIX |
Lost |
DLBCL |
223 |
C |
| 11-SBL |
female |
77 |
Right |
uncertain |
No |
IV stage Agroup |
33 montds # |
DLBCL |
>2150 |
C |
| 12-SBL |
female |
45 |
Left |
uncertain |
Yes |
IV stage Agroup |
Lost |
DLBCL |
204 |
C |
| 13-SBL |
female |
76 |
bilateral |
uncertain |
No |
IV stage Agroup |
17 montds* |
DLBCL |
349 |
C |
| 14-SBL |
female |
71 |
bilateral |
uncertain |
No |
IV |
10 montds* |
DLBCL |
246 |
C |
| 15-SBL |
female |
39 |
Left |
uncertain |
No |
IV |
54 montds # |
FL |
544.95 |
C |
| 16-SBL |
female |
50 |
bilateral |
uncertain |
No |
IVb |
6 montds * |
PTCL |
242 |
C |
| Case Type |
Specific treatment programs |
WBCcount |
ki67% |
BMI |
| 1-PBL |
COEP regimenchemotderapy 7 cycles+ chest wall radiotderapy |
6.53 |
60% |
21.48 |
| 2-PBL |
R-CHOP regimenchemotderapy + radiotderapy to tde cervical lymph node region |
1.8 |
90% |
18.36 |
| 3-PBL |
COEP1 cycle + CHOP7 cycle,R-ICE regimen 5 cycles, left breast and axillary lymphnode radiotderapy 25 times, righteye radiotderapy 25 times, R-CVP regimen targeted combinedchemotderapy 3 cycles. |
Null |
70% |
23.43 |
| 4-SBL |
R-CHOP Program 5 Cycles |
6 |
75% |
20.54 |
| 5-SBL |
CHOP regimenchemotderapy 7 times,R-GDP regimen chemotderapy 6 times, stemcell transplantation. |
5.48 |
Null |
22.18 |
| 6-PBL |
One cycleof R-CHOP chemotderapy |
3.33 |
Null |
20.81 |
| 7-PBL |
Not treatedat tdis hospital |
2.69 |
80% |
23.43 |
| 8-PBL |
R-CHOP regimen, DICE regimen 5 cycles, GEMO1 cycle. |
5.13 |
80% |
29.29 |
| 9-SBL |
COEP-L regimen chemotderapy 4 cycles, GDP+ lenalidomide 1 cycle + MTX + cytarabine intratdecal injection. Triptoril monoclonal antibody immunotderapy |
9.69 |
60% |
24.03 |
| 10-SBL |
R-CHOP regimen was used for 6 cycles, and IP regimen was used for 1 cycle |
3.67 |
+ 75% |
26.67 |
| 11-SBL |
R-CHOP regimenwas used for 8 cycles, and COP regimen was used for 14 cycles |
6.48 |
Lack |
24.97 |
| 12-SBL |
R-CHOP chemotderapy for 7 cycles |
4.8 |
90% |
28.8 |
| 13-SBL |
R-COP regimen was used for 2 cyclesof chemotderapy, andR-GDP regimen wasused for 2 cycles of chemotderapy |
5.14 |
Lack |
22.13 |
| 14-SBL |
One cycleof vincristine, 7 cycles of CHOP chemotderapy |
2.33 |
Lack |
19.7 |
Note: C: Chemotherapy; T: Targeted therapy; R: Radiotherapy; S: Stem cell transplantation; *Patient death; #Follow-up deadline.
Short-term curative effect
Among the 16 patients, 3 receiving chemotherapy received PR, and the rest continued to change their treatment regimen because the therapeutic effect was not sustained. Overall survival in PBL was higher than that in SBL (194>170 months). Of these 16 patients, only one patient had low ki67 expression and the rest had high ki67 expression among known numerical cases. Low expression of ki67 ranged from 3 to 30%, with OS of 6 months. In highly expressed ki67 cases, the lowest was 60%, with OS at 32 months and 44 months, respectively; The highest was 90% for ki67 and 8 months for OS.
Survival analysis
Up to June 30, 2023, the median follow-up was 25 months (3-82 months), and the median survival time was 25 months. The 2-year overall survival rate was 56.25%, the 3-year overall survival rate was 43.75%, and the 5-year overall survival rate was 25%.
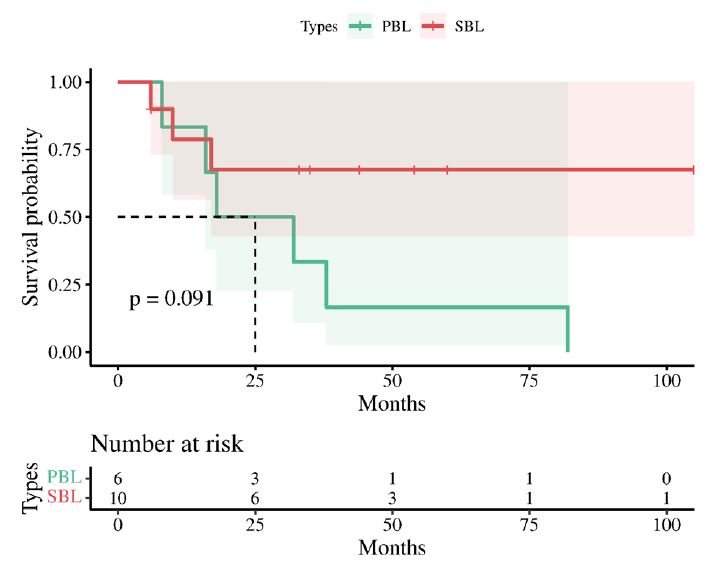
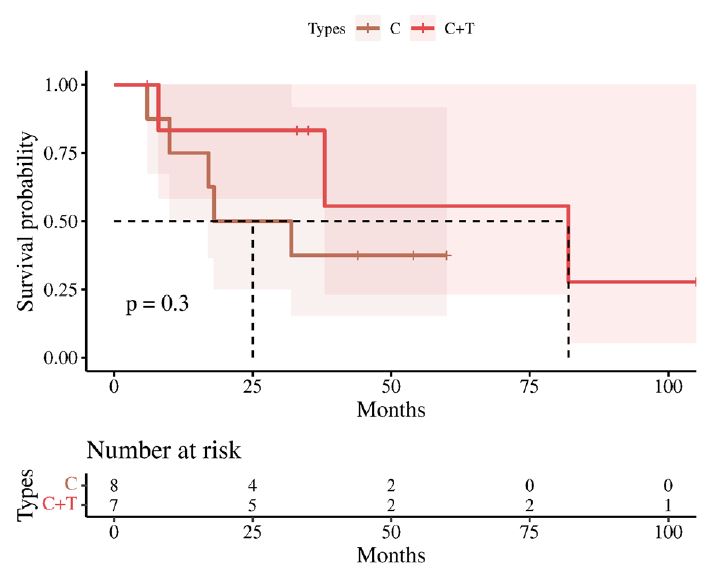
Kaplan-Meier analysis results showed that the survival curve of 16 patients with pathological follow-up data is shown in (Figure 1). The survival analysis results of PBL and SBL were shown in (Figure 2), P>0.05, and there was no significant difference between them in survival analysis. The survival analysis results of chemotherapy and combined chemotherapy targeting were shown in (Figure 3), P>0.05, and there was no significant difference in survival analysis between the two.
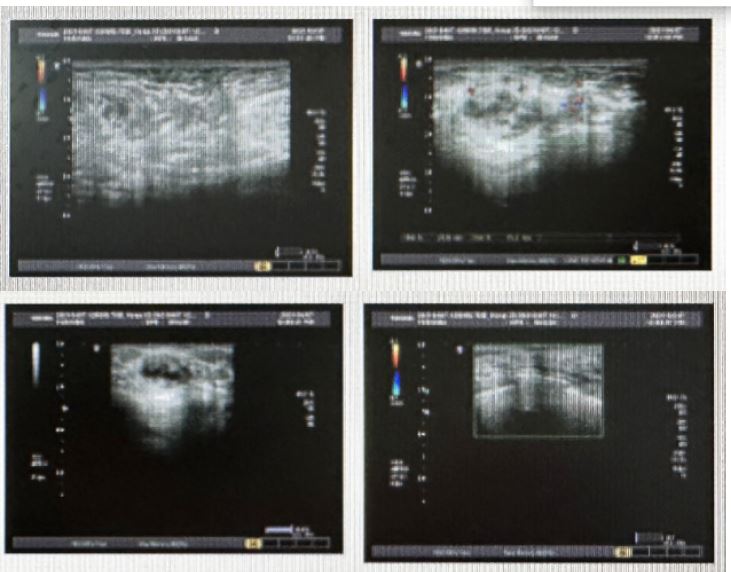
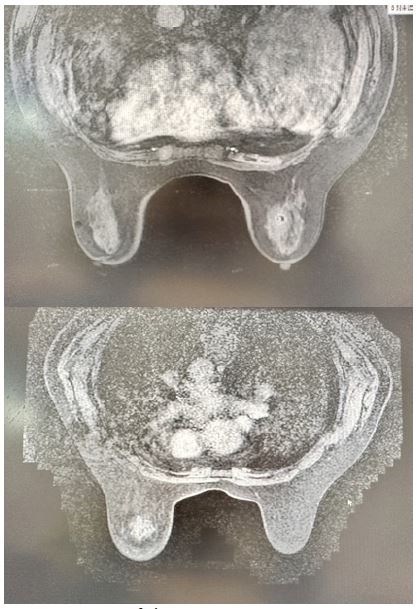
Clinical imaging analysis
The B-ultrasound features of 16 BL patients were non-specific, with oval or irregular mass morphology, blurred borders, and low or mixed echo Figure 4). In 16 cases, mammography showed nonspecific lesion edges, which were usually unclear and had less burr edges, and less obvious skin thickening and lymphedema, which were mainly characterized by high-density mass shadows. The MRI of 1 BL patient was similar to that of breast cancer, usually with a round or oval mass. T1-weighted imaging showed low or equal intensity in some areas, and T2-weighted imaging showed high intensity (Figure 5).
Discussion & conclusion
BL is a rare solid type tumor, mainly classified as PBL or SBL, and its clinical manifestations are similar to breast cancer, usually including a breast mass with or without ipsilateral axillary lymph node enlargement. PBL accounts for less than 1% of breast malignancies and less than 2% of NHL [14]. PBL is more aggressive and has a worse prognosis than other sites of extratodular NHL, such as the gastrointestinal tract [15]. SBL is clinically rare, occurring in only 0.07% of cases, but is the most [16] common tumor to metastasize to the breast, accounting for 17% of secondary breast metastases.
Primary and secondary lymphomas are two distinct lymphatic system malignancies that differ in origin and clinical presentation, but share some common therapeutic challenges and goals. Primary lymphomas originate within the lymphatic system, such as the lymph nodes, spleen, etc., while secondary lymphomas spread into the lymphatic system from sites outside the lymphatic system, such as solid organs. Symptoms of primary lymphoma usually include painless enlargement of the lymph nodes, fever, and weight loss, while secondary lymphoma may be accompanied by symptoms related to the primary site. Although the two may differ in treatment, including chemotherapy, radiation, targeted therapy, and hematopoietic stem cell transplantation, both aim to control the disease, relieve symptoms, improve quality of life, and prolong survival. In addition, both diagnoses need to be confirmed by biopsy and pathology, and both may face challenges with drug resistance, relapse, and treatment-related complications during treatment.
PB-DLBCL is a rare and potentially curable disease with symptoms similar to those of other breast malignancies. PB-DLBCL occurs mostly in women and is rare in men. In Asian countries, the age of onset is 45-53 years [17]. In this study, all patients were female, and the median age of onset was 64 years old. Diffuse large B-cell lymphoma was the dominant pathological type (11/16 cases), which was similar [6] to previous studies. PB-DLBCL is usually characterized by a painless breast mass, which occurs in 61% of patients. It is unilateral or bilateral breast mass, most of which is unilateral breast disease, the incidence of the right side is more than that of the left side, and the lesions are mostly located in the upper quadrant [18,19] of the outer breast. A small number of PB-DLBCL patients were accompanied by B symptoms such as fever, night sweats and weight loss. Ipsilateral axillary lymph nodes were involved in 40%-50% [6] of patients. All the patients in this study had painless breast mass as the initial symptom; 8 cases were accompanied by ipsilateral axillary lymph node invasion; 4 patients were accompanied by B symptom, which was consistent [3,6,18,19] with existing literature reports.
Due to the low incidence of PB-DLBCL, the small number of patients in related studies, the long period, and the different treatment methods, the standard treatment plan has not been established. At present, the role of surgery in the treatment of PB-DLBCL remains controversial. Most scholars [3,3,19] believe that mastectomy can not improve the survival and prognosis of PB-DLBCL patients. The possible reasons are that surgery, especially radical resection incision healing time is longer and patients’ mental trauma is increased, which affects the timely implementation of chemotherapy and radiotherapy and thus affects the therapeutic effect. Jennings et al. [11] included 465 patients with PBL in their study, and found that mastectomy did not bring survival benefits to patients, but was associated with higher all-cause mortality and disease-related mortality. Caon et al. [20] ‘s study also confirmed that 5-year OS rates were 40.5% and 20.5% for PB-DLBCL patients in IE and IIE stages who received surgical treatment alone. Among the 16 patients in this study, 7 patients received surgery, and no surgical treatment was found to prolong the patients’ OS and PFS. Therefore, it is generally believed that surgical treatment has no clear benefit and is usually only used for diagnosis, rather than recommended for the treatment of SBL. However, because the clinical presentation of PB-DLBCL is sometimes indistinguishable from breast cancer, most patients first undergo therapeutic surgery before a definitive diagnosis is made. Systemic chemotherapy remains the cornerstone of PB-DLBCL treatment, with anthracycline-based chemotherapy regimens such as CHOP being used. The IELSG-15 study found that combined anthracycline [3,18] therapy prolonged PFS and OS in PB-DLBCL patients, and patients treated with less than four cycles of anthracycline had a worse prognosis than those treated with full chemotherapy. Systemic chemotherapy of more than 3 cycles [5] has also been found to improve disease-related survival in PBL patients. This study found no survival benefit for patients with PB-DLBCL with more than 6 cycles of chemotherapy.
Radiotherapy consolidates the effects of systemic chemotherapy, but the role of radiotherapy in PBDLBCL patients is unclear. The target areas of radiotherapy usually include the affected mammary gland, chest wall, and armpit. The use of conventional radiotherapy for the opposite mammary gland is still controversial. Jenings WC et al. [21] proposed in their study that for patients with stage I PB-DLBCL, the risk of recurrence is lower than that of patients receiving chemotherapy alone regardless of whether radiotherapy is combined with chemotherapy (P=0.037). A similar conclusion was reached in the study by Aviles A et al. [22]. Patients receiving the CHOP regimen combined with radiotherapy had longer OS than those receiving chemotherapy alone. The IELSG-15 study [3] also found that patients in the chemotherapy plus radiotherapy plus surgery group had longer OS than those in both the chemotherapy plus radiotherapy plus surgery group and the radiotherapy plus surgery group (P=0.001), suggesting that anthracycline-containing chemotherapy plus radiotherapy may be the best treatment modus operas for PB-DLBCL patients. The differences in PFS and OS between patients who received radiotherapy and those who did not in this study were not statistically significant. However, the sample size of this study was small and the grouping was unbalanced, so the therapeutic status of radiotherapy in PB-DLBCL needs to be further explored. The recurrence of PBL was most common in the central region, with an incidence of 14.0%-21.0%. The recurrence rate of central nervous system was higher in PB-DLBCL patients, which was 12.0%-27.0% [23]. However, it is still controversial whether to carry out central prophylactic chemotherapy regularly. It is of guiding significance to explore the high-risk factors of central relapse. Hosein et al [10]. found that IIE stage and stage-adjusted IPI (sa-IPI) may be a risk factor for central relapse in PB-DLBCL patients, but the difference was not statistically significant, which may be the reason for the small sample size. At present, the prevention methods of central recurrence of PB-DLBCL include HD-MTX and intrathecal injection, but the relevant literature is limited. Some studies [10] have found that the difference in central recurrence rate between PB-DLBCL patients who received central prophylactic injection and those who did not receive central prophylaxis is not statistically significant. At present, no large-scale prospective study has confirmed the central prophylaxis effect of chemotherapy combined with HD-MTX in PB-DLBCL patients. Of the 16 patients in this study, 1 patient received cytarabine intrathecal injection, and none of the patients experienced central recurrence. Current studies [3,6,8,10] have disputed the prognostic factors of PB-DLBCL. Most of them believe that age, IPI score, baseline LDH level, tumor length and Ann Arbor stage are independent prognostic factors of patients.
To sum up, SBL is a relatively rare disease, and large-scale prospective studies are lacking at present. Although systematic chemotherapy combined with surgery or radiotherapy is the usual treatment regimen, no consensus has been reached on its standard first-line treatment mode. This study mainly affirms the therapeutic value of conventional chemotherapy regimens in PBL and SBL. However, there are some limitations in this study. As a retrospective study, there is a certain degree of bias in the selection of cases and data. In addition, the included cases in this study were from a single center with a small sample size, so it is still necessary to further explore the prognostic factors and the optimal treatment mode of PBL and SBL in a large sample prospective study, so as to provide a theoretical basis for the treatment of SBL.
Abbreviations: BC: Breast Cancer; SBL: Secondary Breast Lymphoma; PBL: Primary Breast Lymphoma; DLBCL: Diffuse Large B Cell Lymphoma; BCL: B Cell Lymphoma; FL: Follicular Lymphoma; PTCL: Peripheral T-Cell Lymphoma; NK/TL: Nk/T Cell Lymphoma; MCL: Mantle Cell Lymphoma; R-CHOP Regimen: Rituximab + Doxorubicin Liposome + Cyclophosphamide + Vindesine; IP: Ifosfamide+Cisplatin; R-ICE: Rituximab 375 mg/M2 600 mg D0, Ifosfamide 2 g D2, Carboplatin 300 mg/M2 480 mg D2,VP-16 100 mg/M2 0.1gd1-3q 21d; CHOP: Cyclophosphamide+Vincristine+Adriamycin + Prednisone; VP: Vincristine + Prednisone Acetate; CVP: Cyclophosphamide + Vincristine + Prednisone Acetate; ECHOP: Cyclophosphamide + Vincristine + Etoposide + Epirubicin + Prednisone Acetate; Gemox: Gemcitabine + Oxaliplatin; R-ICE: Rituximab 375 mg/M2 600 mg D0, Ifosfamide 2 g D2, Carboplatin 300 mg/M2 480 Mg D2, VP-16 100 Mg / M2 0.1 g D1-3q 21d; R-CVP: Rituzumab,Cyclophosphamide, Vincristine, Prednisone.
Funding: No funding.
Conflicts of interest: The authors declare no conflict of interest.
References
- Xia C, Dong X, Li H, et al. Cancer statistics in china and United States. Profiles, trends, and determinants J. Chinese Medical Journal. 2022; 135(5): 584-590. DOI: 10.1097 / CM9.0000000000002108.
- Shim E, Song SE, Seo BK, et al. Lymphoma affecting the breast: A pictorial review of multimodal imaging findings J. Journal of Breast Cancer. 2013; 16(3): 254-265 DOI: 10.4048 / JBC. 2013.16.3.254.
- Ryan G, Martinelli G, Kuper-Hommel M, et al. Primary diffuse large b-cell lymphoma of the breast: Prognostic factors and outcomes of a study by the international extranodal lymphoma study group J. Annals of Oncology. 2008; 19 (2): 233-241. The DOI: 10.1093 / annonc/mdm471.
- Ganjoo K, Advani R, Mariappan MR, et al. Non-hodgkin lymphoma of the breast J. Cancer. 2007; 110(1): 25-30. DOI:10.1002/cncr.22753.
- Domchek SM, Hecht JL, Fleming MD, et al. Lymphomas of the breast J. Cancer. 2002; 94(1): 6-13. DOI:10.1002/cncr.10163.
- Aviv A, Tadmor T, Polliack A. Primary diffuse large b-cell lymphoma of the breast: Looking at pathogenesis, clinical issues and therapeutic options J. Annals of Oncology. 2013; 24(9): 2236-2244. DOI: 10.1093 / annonc/mdt192.
- Surov A, Holzhausen HJ, Wienke A, et al. Primary and secondary breast lymphoma: Prevalence, clinical signs and radiological features J. The British Journal of Radiology. 2012; 85(1014): E195 - e205. DOI: 10.1259 / BJR / 78413721.
- Jeanneret-Sozzi W, Taghian A, Epelbaum R, et al. Primary breast lymphoma: Patient profile, outcome and prognostic factors. A multicentre rare cancer network studyJ.. BMC Cancer. 2008; 8: 86. DOI:10.1186/1471-2407-8-86.
- Uesato M, Miyazawa Y, Gunji Y, et al. Primary non-hodgkin’s lymphoma of the breast: report of a case with special reference to 380 cases in the japanese literature J. Breast Cancer. 2005; 12(2): 154-158. DOI:10.2325/jbcs.12.154.
- Hosein PJ, Maragulia JC, Salzberg MP, et al. A multicentre study of primary breast diffuse large b-cell lymphoma in the rituximab era J. British journal of Haematology. 2014; 165(3): 358-363. DOI:10.1111/bjh.12753.
- Jennings WC, Baker RS, Murray SS, et al. Primary breast lymphoma J. Annals of Surgery. 2007; 245(5): 784-789. The DOI: 10.1097/01. Sla. 0000254418.90192.59.
- Leyvraz S, Burckhardt P. Radionuclide targeting of bone metastases: Which efficacy? J. Journal of Clinical Oncology. 1990; 8(9): 1598-1599. The DOI: 10.1200 / JCO 1990.8.9.1598.
- Cheson BD, Pfistner B, Juweid ME, et al. Revised response criteria for malignant lymphomaJ.. Journal of Clinical Oncology. 2007; 25(5): 579-586. DOI: 10.1200 / JCO 2006.09.2403.
- Duncan VE, Reddy VVB, Jhala NC, et al. Non-hodgkin’s lymphoma of the breast: A review of 18 primary and secondary cases J. Annals of Diagnostic Pathology. 2006; 10(3): 144-148. DOI: 10.1016 / j.a nndiagpath. 2005.09.018.
- Jennings WC, Baker RS, Murray SS, et al. Primary breast lymphoma J. Annals of Surgery. 2007; 245(5): 784-789. The DOI: 10.1097/01. Sla. 0000254418.90192.59.
- Zagouri F, Sergentanis TN, Nonni A, et al. Secondary breast lymphoma diagnosed by vacuum-assisted breast biopsy: A case report J. Journal of Medical Case Reports. 2007; 1: 113. DOI:10.1186/1752-1947-1-113.
- Jennings WC, Baker RS, Murray SS, et al. Primary breast lymphoma J. Annals of Surgery. 2007; 245(5): 784-789. The DOI: 10.1097/01. Sla. 0000254418.90192.59.
- Yhim HY, Kang HJ, Choi YH, et al. Clinical outcomes and prognostic factors in patients with breast diffuse large b cell lymphoma; consortium for improving survival of lymphoma (cisl) study J. BMC Cancer. 2010; 10: 321. DOI:10.1186/1471-2407-10-321.
- Validire P, Capovilla M, Asselain B, et al. Primary breast non-hodgkin’s lymphoma: A large single center study of initial characteristics, natural history, and prognostic factors J. American Journal of Hematology. 2009; 84(3): 133-139. (in Chinese) DOI:10.1002/ajh.21353.
- Caon J, Wai E S, Hart J, et al. Treatment and outcomes of primary breast lymphoma J. Clinical Breast Cancer. 2012; 12(6): 412-419. The DOI: 10.1016 / j.carol carroll LBC. 2012.07.006.
- Wiseman C, Liao KT. Primary lymphoma of the breast J. Cancer. 1972; 29(6): 1705-1712. DOI:10.1002/1097-0142(197206)29:6<1705::AID-CNCR2820290640>3.0.CO; 2-I.
- Aviles A, Neri N, Nambo MJ. The role of genotype in 104 cases of diffuse large b-cell lymphoma primary of breastJ.. American Journal of Clinical Oncology. 2012; 35 (2): 126. DOI: 10.1097 / COC. 0 b013e318209aa12.
- Gholam D, Bibeau F, El Weshi A, et al. Primary breast lymphoma J. Leukemia & Lymphoma. 2003; 44(7): 1173-1178. DOI: 10.1080/1042819031000079195.