Introduction
Colorectal Cancer (CRC) remains a global health issue with more than 1.3 million patients diagnosed with CRC yearly and an estimated more than 600.000 deaths [1]. Hematogenous metastatic spread is a major concern as around 50% of patients will develop distant metastases at some point during the treatment course. The natural history of the metastatic spread has been described in autopsy studies, reporting liver and lungs as the most frequent sites of dissemination [2].
Adrenal metastases are common for other malignancies especially lung cancer and breast cancer with incidences ranging from 20-30% [3]. For colorectal cancer, a historic autopsy study of 457 patients with colorectal adenocarcinoma revealed adrenal metastases in 63 cases (14%) of which 29 had bilateral involvement (6%) [4]. However, the incidence of isolated adrenal metastases, hence no extra-adrenal disease, has not been reported in the literature.
Treatment of adrenal metastases is complex as this is most often part of a multifocal clinical picture with other metastatic sites. Since the first report of successful unilateral adrenalectomy for metastatic cancer in 1982 [5], there has been published several case series reporting prolonged survival after surgical treatment of solitary adrenal metastases [6,7]. Resection of bilateral adrenal metastases is more controversial as the effect on overall survival is unclear and the procedure will with certainty leave the patient with adrenal insufficiency.
Here, we report an unusual case of a patient undergoing left and subsequent right sided adrenalectomy for metachronous metastases from a previously resected rectal adenocarcinoma.
Case report
In April 2019, a previously healthy 73-year-old man presented with a history of altered bowel movement and fecal incontinence. Colonoscopy showed a mid-rectal tumor and biopsy confirmed the diagnosis adenocarcinoma with KRAS mutation and microsatellite stable genotype. A Magnetic Resonance scan demonstrated a T3N2V2 tumor with enlarged lymph nodes <1 mm from the mesorectal fascia. A Positron Emission Tomography (PET) scan showed 4 PET-positive lymph nodes in close proximity to the rectal tumor but no evidence of distant metastases. P-Carcinoembryonic Antigen (CEA) level was low (<4 mg/L).
According to the Danish national guidelines treatment consisted of neoadjuvant external beam radiotherapy delivering 50.4 Gy in 28 fractions with concomitant capecitabine (850 mg/m2).
Nine weeks after completing CRT the patient underwent a total mesorectal excision with no post-operative complications. Pathology revealed an ypT3ypN1 rectal adenocarcinoma. No adjuvant chemotherapy was given.
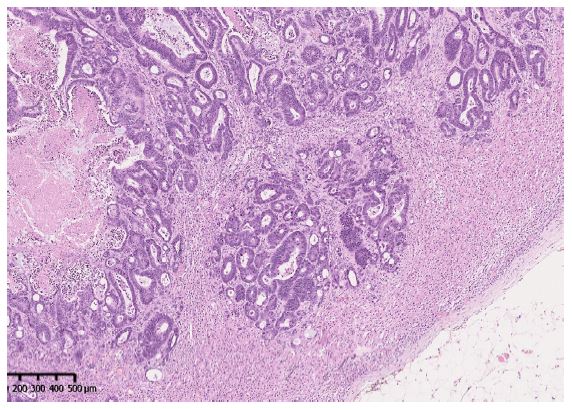
During follow-up, a routine performed Computer Tomography (CT) scan 15 months after surgery revealed a mass in the left adrenal gland. A laparoscopic left-sided adrenalectomy was performed. Pathology showed a 35 x 20 x 48 mm sized adenocarcinoma placed centrally in the adrenal gland. Immunohistochemistry showed expression of CK20, SATB-2 and CDX-2 (Figure 1). This confirmed the presence of a metastatic lesion from the previously resected rectal cancer. Adrenalectomy was followed by 8 cycles of capecitabine (2500 mg/m2) as adjuvant therapy and follow-up CT scans every 3 months.
In October 2021, 6 months after completion of adjuvant chemotherapy, a CT scan showed a new mass in the right adrenal gland. A PET scan was performed showing no signs of metastasis elsewhere and following multidisciplinary discussion, the patient underwent a right-sided adrenalectomy. Pathology showed a 12 x 8 x 12 mm tumor with immunohistochemistry confirming a new metastasis from the patients previously resected rectal adenocarcinoma.
No adjuvant chemotherapy was administered after the second adrenalectomy. A follow-up schedule with regular CT scans every three months was initiated. As of June 2024 the patient remains disease free.
Following bilateral adrenalectomy, the patient was referred to the Department of Endocrinology for management of adrenal insufficiency. He is currently treated with Hydrocortisone 15 + 5 mg and Florinef (Fludrocortisone) 0.05 mg daily. On this treatment, the patient is normotensive with normal biochemistry. He is well-being and physically active.
Table 1: Retrieved cases of patients with resected bilateral adrenal metastases from colorectal adenocarcinoma.
| Author |
Country |
Year |
Primary tumor |
Mutation status |
Curative intention |
| Pedersen et al. |
Denmark |
2023 |
Rectal |
KRAS mutation |
yes |
| Tsujimoto et al. [12] |
Japan |
2019 |
Rectal |
Unknown |
yes |
| Tsujimoto et al. [12] |
Japan |
2019 |
Sigmoid |
Unknown |
yes |
| Liu et al. [13] |
China |
2015 |
Sigmoid |
Unknown |
yes |
| Jabir et al. [14] |
Morocco |
2014 |
Rectal |
Unknown |
yes |
| Thrumurthy et al. [15] |
England |
2011 |
Sigmoid |
Unknown |
yes |
| Crisci et al.[16] |
Italy |
2000 |
Sigmoid |
Unknown |
yes |
Discussion
Over the past decades, metastatic Colorectal Cancer (mCRC) has become a complex treatment landscape with increasingly use of various local treatment modalities (resection, ablation, stereotactic body radiation) for patients presenting with an oligometastatic phenotype [8]. This trend of increasingly use of surgical treatment of metastases has also been documented for rare metastatic sites including the central nervous system and adrenal glands [9].
In the present case, we report the clinical course of a patient who developed metachronous metastases in both adrenal glands from a previously resected rectal cancer. Our patient had a disease-free interval of one year between the recognition of the right and left adrenal metastases and has never presented with any extra-adrenal disease.
Following multidisciplinary team discussion, it was decided to offer this patient surgical treatment of the adrenal metastases. This was supported by 1) the lack of visual extra-adrenal disease (on CT and PET scans), 2) the apparent indolent biological nature of the disease and 3) the patient preference and patient characteristic being in good general health and WHO Performance Status 0. After the first laparoscopic adrenalectomy the patient was offered adjuvant chemotherapy with single agent capecitabine (2500 mg/m2) for a duration of 6 months. Systemic therapy was chosen as the patient had only been exposed to concomitant capecitabine during the preoperative chemo-radiation.
The prognosis following adrenal metastasectomy is discussed in a recent nationwide Danish population- based study [10]. Here, 435 patients with various primary tumors were followed up after adrenal metastasectomy describing a 5-year overall survival of 31%. This study identified negative prognostic markers e.g. non-radical procedure and lung cancer. Furthermore, adrenal metastases have been proposed as a possible sanctuary site for systemic therapy [11], thus advocating for a surgical approach when possible.
Management of bilateral adrenal metastases is challenging and optimal patient selection for surgery is critical. We have reviewed the literature seeking to identify all published cases of bilateral adrenalectomy for isolated colorectal cancer metastases. We found only 5 other publications reporting clinical data for 6 patient courses (Table 1) [12-16]. Interestingly, all cases had primary tumor in the left side of colorectal anatomy, either as a primary rectal or sigmoid cancer. The sidedness of the primary tumor in colorectal cancer (left sided versus right sided) has been shown to hold prognostic and predictive value in mCRC [17].
We hypothesize, that both biological differences between right and left sided primary tumors as well as the extrahepatic venous drainage from low rectal cancer could contribute to this apparent observation. Our case is the only reporting the mutational status of the primary tumor concerning the oncogenes KRAS, NRAS and BRAF. The presence of a KRAS mutation in colorectal adenocarcinoma has previously been associated with a different pattern of metastases including a higher risk of brain metastases [16].
Adrenal insufficiency is an obvious consequence following bilateral adrenalectomy. However, adrenal failure has also been described due to adrenal metastases without surgical resection [17]. Lifelong medication with glucocorticoid and mineralocorticoid substitution and surveillance by endocrinologist is warranted, including patient education with emphasis on the need for extra glucocorticoid treatment in case of intercurrent illness.
Conclusion
In conclusion, isolated bilateral adrenal metastases from colorectal cancer is a very rare clinical entity only described in case series. Her, we report a favorable outcome following combined modality treatment of rectal cancer with metachronous bilateral adrenal metastases. Multidisciplinary management with oncologists, endocrinologists and surgeons is critical for an optimal clinical course.
References
- Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN. Int J Cancer. 2015; 136: E359-E386.
- Weiss L, Grundmann E, Torhorst I, Hartveit F, Moberg I, et at. Haematogenous metastatic patterns in colonic carcinoma: An analysis of 1541 necropsies. J Pathol. 1986; 150(3): 195-203.
- Tallis PH, Rushworth RL, Torpy DJ, et al. Adrenal insufficiency due to bilateral adrenal metastases- A systematic review and meta-analysis. Heliyon. 2019; 5: e01783.
- BJ Cedermark, LE Blumenson, JW Pickren, et al. Ths significance of metastases to the adrenal glands in adenocarcinoma of the colon and rectum. Surg Gynecol Obstet. 1977; 144(4): 537-46.
- Twomey P, Montgomery C, Clark O. Successful treatment of adrenal metastases from large-cell carcinoma of the lung. JAMA. 1982; 248: 581-3.
- Puccini M, Panicucci E, Candalise V, et al. The role of laparoscopic resection of metastases to adrenal glands. Gland Surg. 2017; 6(4): 350-354.
- Marangos IP, Kazaryan AM, Rosseland AR, et al. Should we use laparoscopic adrenalectomy for metastases? Scandinavian multicenter study Journal of Surgical Oncology. 2009; 100(1): 43-7.
- Boysen AK, Spindler KL, Høyer M, et al. Metastases directed local treatment for colorectal cancer- a 14 years nationwide experience. Int J Cancer. 2018.
- Bartlett E, Simmons K, Wachtel H et al. The rise in metastasectomy across cancer types over the past decade. Cancer. 2015; 747-757.
- Vlk E, Ebbehoj A, Donskov F, et al. Outcome and prognosis after adrenal metastasectomy: Nationwide study, BJS OPEN. 2022.
- Cohen R, Jonchere V, Fouchardiere C, et al. Adrenal gland as a sanctuary site for immunotherapy in patients with microsatellite instability-high metastatic colorectal cancer. Journal for immunotherapy of cancer. 2021; 9: e001903.
- Tsujimoto A, Ueda T, Kuge H, et al. Long-term survival after adrenal metastasectomy from colorectal cancer: A report of two cases Surg Case Rep. 2019; 5(1): 61
- Liu Y, Chen Z, Zhai ET, et al. Case of metachronous bilateral isolated adrenal metastasis from colorectal adenocarcinoma and review of the literature World J Gastroenterol. 2016; 22(14): 3879-84.
- Jabir H, Tawfiq N, Moukhlissi M, et al. Metachronous bilateral isolated adrenal metastasis from rectal adenocarcinoma: A case report Case Rep Gastrointest Med. 2014; 2014: 516403.
- Thrumurthy SG, Jadav AM, Pitt M, et al. Metachronous bilateral adrenal metastases following curative treatment for colorectal carcinoma Ann R Coll Surg Engl. 2011; 93: e96-e98.
- Criscia A, Carteib G, Antonia PD, et al. Surgical Management of Isolated Bilateral Adrenal Metastases from Colon Carcinoma Causing Adrenal Insufficiency Urol Int. 2001; 67: 113-116.
- N Boeckx, R Koukakis, K Op de Beeck, et al. Primary tumor sidedness has an impact on prognosis and treatment outcome in metastatic colorectal cancer: results from two randomized first-line panitumumab studies. Ann Oncol. 2017; 28(8): 1862-1868.
- Christensen TD, Spindler KL, Nielsen D. Systematic review: Brain metastases from colorectal cancer-Incidence and patient characteristics BMC Cancer. 2016; 16: 260.
- Imaoka Y, Kuranish F, Ogawa Y, et al. Adrenal failure due to bilateral adrenal metastasis of rectal cancer: A case report Int J Surg Case Rep. 2017; 31: 1-4.