Case presentation
The patient was a 66-year-old woman admitted to the hospital
with abdominal pain for 4 days. She had persistent vague pain in
the abdomen with slight abdominal distension. She had regular
menstruation and menopause at the age of 43, and had 6 pregnancies and 5 deliveries. The patient had no other past medical
history.
Physical examination: No enlargement of superficial lymph
nodes, abdominal compressions are slightly painful. Gynecologic examination: old perineal laceration of II°, senile changes of
vulva, no ulceration, no superfluous growths, and the vagina is
unobstructed. The uterus was normal in size, with good mobility.
A 7 cm diameter mass was found in both adnexa. Both ovarian
fallopian tubes have palpable masses of about 7 cm in diameter,
and the surface of the right mass is nodular, movable, and mildly
tender.
Laboratory examination: Ultrasound in obstetrics and gynecology, 5.6 × 4.7 × 4.9 cm and 7.0 × 3.9 × 5.2 cm solid hypoechoic
masses were seen in the left and right adnexal areas, respectively, with irregular morphology and internal blood flow signal. Barium
enema colonography, localized stenosis in the proximal part of
the ascending colon, considering the possibility of tumor invasion.
The whole abdomen CT showed: The mass is in the bilateral
adnexal area, right lower abdomen or retroperitoneal masses, bilateral multiple enlarged lymph nodes, thickening of the omentum around the right colon, considering: malignant tumor in the
adnexal area, the rest are multiple metastases; malignant mesenchymal tumor in the right lower abdomen, the rest are metastases.
Hematology: white blood cells are normal (6.42 × 10
9 /L),
Hemoglobin is lowered (114.0 g/L), elevated platelet count (305 ×
10
9/L), decreased lymphocyte percentage (0.17). Elevated CA125
(54.7U/ml).
Ascites: Malignant tumor cells.
Surgical treatment seen in the abdominal cavity: about 50 ml
of clear ascites, the bilateral ovaries were solidly enlarged, grayish
white, the left ovarian mass was about 7 cm, the right ovarian
mass was about 5 cm, the solid mass protruded retroperitoneally,
adhered to the ipsilateral pelvic wall and uterus. A solid mass of
about 6 × 6 cm in size was seen in the mesentery near the root
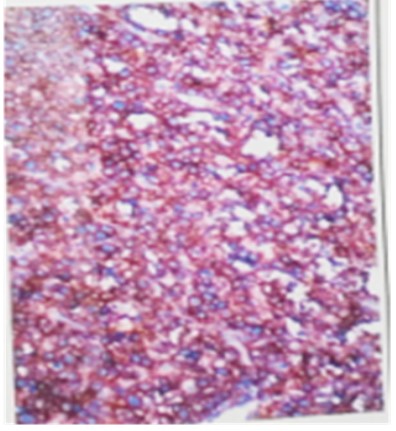
of the colon, which was tough with clear borders and did not involve the intestinal lumen. The frozen section showed a malignant ovarian mass tumor. Postoperative pathology showed diffuse large B-cell lymphoma of the ovary, non-specific (germinal
center type), tumor involvement in the bilateral parametrium,
bilateral paracervical, bilateral fallopian tubes, vaginal stump and
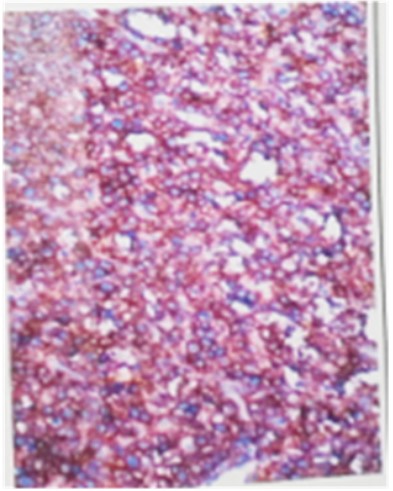
cervical canal. Immunohistochemistry showed: CD20(++); CD3(-); Ki-67(80%+); CD56(-); CD99(-); CgA(-); CK(-); CK7(-); EMA(-); Inhibin-a(-); SALL4(-); Syn(-); Vimentin(-); WT-1(-) (Figure 1) (Small
mesentery). Diffuse large B-cell lymphoma, germinal center origin, immunohistochemistry showed: CD20(+); CD79a(+); PAX-5(+); CD5(-); CD3(-); CD30(-); CD38(partial +); CD10(+); MUM1(+);
Bcl-6(+); P53(+); ALk(-); CD15(-); CK(-); cyclinD1(-); EMA(-); GranzymeB(-); TIA-1(-); c-Myc(-); Ki-67(80%+) (Figure 2). Tumor was
detected in mesenteric lymph nodes (10/10).
The Final diagnosis was Stage IV diffuse large B-cell lymphoma
of the ovary. Follow-up treatment was recommended to the oncology department. She was discharged 28 days after surgery, but
was readmitted the hospital due to hypoproteinemia and infected
surgical incision. The patient was cachectic, with multiple complications including cancer cachectic, secondary pernicious anemia,
ureteral fistula, intestinal fistula, and poor healing of the vaginal
stump. A multidisciplinary consultation recommended palliative
treatment. But the patient’s family abandoned the treatment and
she died 3 months after surgery.
Discussion
Etiology and incidence
Lymphoma is a group of malignant tumors arising from lymph
nodes and extra-nodal lymphatic tissue [1]. It is divided into Hodgkin's lymphoma and non-Hodgkin's lymphoma. Which non-Hodgkin's lymphoma is a common type, and it can involve the ovaries,
uterus, cervix, vagina and vulva in the reproductive system. The incidence of ovarian involvement is approximately 7%-30% [2].
Most clinical show with pelvic masses and abdominal pain. The
most common type is Diffuse Large B-cell Lymphoma (DLBCL), and
the most DLBCL is the germinal center type [3]. Since the ovaries
is not contain lymphoid tissue, the ovarian-derived lymphoma is
controversial. Most think that the tumor may originate from lymphocytes around the vascular of hepatic hilum. A few lymphocytes
within the epithelium of teratoma and lymphocytes near the corpus luteum, and originates from follicular central cells [1,4]. It has
also suggested that reactive lymphocytes are involved in the inflammatory response of the reproductive system, allowing them
to transform into malignant tumor cells [5].
Diagnosis
DLBCL occurring in the ovary accounts for about 0.5% of non-Hodgkin's lymphomas and 1.5% of ovarian tumors, Most are secondary to generalized lymphoma, and primary disease is rare
[6]. Lymphoma of the ovary has no typical clinical features, and
it is difficult to distinguish it from ovarian cancer by preoperative
frozen section pathology [7-9].Which is often diagnosis according
to the Postoperative pathology and immunohistochemistry. The
commonly used indicators in DLBCL immunohistochemistry including [5] CD20, CD3, CD5, CD10, Bcl-6, Ki-67, MYC. BCL2 and (or)
BCL6 rearrangements, often called Double-hit Lymphoma, also
has a poor prognosis [19]. Syn and CD99 negativity can be distinguished from Peripheral primitive neuroectoderal tumor. CK(-)
can be distinguished from tumors of Epithelial neoplasms. In this
case, Ki67 >80% positive, this indicates that tumor cells are actively proliferating and poor prognosis [10] However, it has also
been suggested that survival is not related to Ki-67 expression [11].
The differential diagnosis between secondary and primary lymphoma which from ovary is difficult, but this is important for the assessment of treatment and prognosis [14]. Primary tumors are
mostly confined to the ovary, while secondary tumors are mostly
considered to be systemic disease of DLBCL involving the ovary
[12]. Secondary ovarian DLBCL can be divided into two types, (1)
The early stages manifest as unknown extra ovarian disease; (2)
secondary ovarian involvement in disseminated systemic DLBCL
[13]. To diagnose primary lymphoma, systemic lymphatic disease
must be excluded, and early primary ovarian lymphoma usually
has a good prognosis [7]. It has been suggested that MRI of bilateral ovarian masses is a clue to diagnosis of ovarian lymphoma,
and once the disease has spread to the abdomen, the differential
diagnosis between primary and secondary is more difficult [12].
The diagnostic criteria for the diagnosis of primary ovarian lymphoma which proposed by Fox and Langley that most people use
today is that [15], 1) tumor confined to the regional lymph nodes
or accessory organs of the ovary at the time of diagnosis; 2) absence of abnormal cells in the bone marrow or peripheral blood;
3) any extra-ovarian disease must occur within a few months of
the appearance of the ovarian lesion.
In this case, the patient had a normal temperature, no night
sweat, and multiple extra-nodal organ invasions before surgery.
And belonged to stage IV type. At the time of diagnosis, the patient had lymph node involvement in the ovary, and mesentery
involvement with regional lymph node metastases. The patient's
condition changes, and no bone marrow smear is done to determine whether there are abnormal cells in the bone marrow. Therefore, the origin of the disease cannot be clarified.
Treatment
Based on the difficulty of preoperative, it has been suggested
that if intraoperative frozen section is highly suspicious that tumors from the reproductive system, surgeons should continue
the cytoreduction, otherwise further treatment options should be
choose by the final pathological diagnosis [12]. Rituximab in combination with CHOP scheme for Non-Hodgkin is an effective treatment [16]. But, a combination of surgery-based treatment with
radiotherapy is currently used, which is inconsistent with the recommended treatment for DLBCL, and the effect of surgery combined with chemo radiotherapy on patient prognosis is unclear.
Most believe that the combination of surgery and chemotherapy
can prolong the survival of patients [17].
Prognosis
The prognosis of DLBCL is closely related to the age, clinical
stage, lesion extent, histology, systemic symptoms, and lactate
dehydrogenase [12,18]. The patient is older, multiple extra-junctional lesions, these all suggested a poor prognosis. Death due
to multiple organ infections such as intestinal fistula, ureter stoma and hypoproteinemia. Two other cases of ovarian DLBCL in
our gynecology department within a decade. Both of them died
within six months after surgery due to periprocedural complications. Combined with this case, we should strengthen perioperative management so that they can receive chemotherapy.
Conclusion
Diffuse large B-cell lymphoma arising in the ovary is rare, The
incidence of DLBCL in the ovary is low. Most of them are diagnosed by postoperative histopathology, and there are few cases
who only receive chemotherapy, and it is difficult to understand the impact of surgery on the prognosis of patients. We believe
that it is necessary to collect more data in the clinic. For patients
with high clinical suspicion of ovarian DLBCL, the therapeutic value of surgical treatment for the disease is fully explored, and a
more reasonable and perfect comprehensive treatment method
is sought to prolong the survival of patients.
References
- Nasioudis D, Kampaktsis PN, Frey M, Witkin SS, Holcomb K. Primary lymphoma of the female genital tract: An analysis of 697 cases.
Gynecol Oncol. 2017; 145: 305-309.
- Lagoo AS, Robboy SJ. Lymphoma of the female genital tract: current status. Gynecol Pathol. 2006; 25: 1-21.
- Xu H, Duan N, Wang Y, et al. The clinicopathological and genetic features of ovarian diffuse large B-cell lymphoma. Pathology.
2020; 52: 206-212.
- Zhu Hong, Guo Xiangrui, Ma Ling. A case of primary non-Hodgkin
lymphoma of ovary and related literature review. MODERN ONCOLOGY. 2020; 28: 444-447.
- Anagnostopoulos A, Mouzakiti N, Ruthven S, Herod J, Kotsyfakis
M. Primary cervical and uterine corpus lymphoma; a case report
and literature review. Clin Exp Med. 2013; 6: 298-306.
- Senol T, Doger E, Kahramanoglu I, et al. Five cases of non-hodgkin B-cell lymphoma of the ovary. Case Rep Obstet Gynecol. 2014;
2014: 392758.
- Li PC, Lim PQ, Hsu YH, Ding DC. Ovarian Diffuse Large B-cell Lymphoma Initially Suspected Dysgerminoma Managed by Laparoscopic Staging Surgery. Gynecol Minim Invasive Ther. 2020; 9: 162-
165.
- Wang Q, Rodriguez R, Marcus JZ, Podolsky L, Campbell D, Heller D.
Pitfalls of Frozen Section in Gynecological Pathology: A Rare Case
of Ovarian Lymphoma in an HIV-Positive Woman Resembling Dysgerminoma on Frozen Section. Surg Pathol. 2019; 27: 387-389.
- Iizuka N, Ikura Y, Fukuoka Y, et al. Malignant Lymphoma of the
Ovary: A Diagnostic Pitfall of Intraoperative Consultation. Gynecol
Pathol. 2020; 39: 79-83.
- Sanchez E, Chacon I, Plaza MM, et al. Clinical outcome in diffuse
large B-cell lymphoma is dependent on the relationship between
different cell-cycle regulator proteins. Clin Oncol. 1998; 16: 1931-
1939.
- Baran M, Canoz O, Altuntas H, et al. Immunohistochemical investigation of P16, P53 and Ki-67’s prognostic values in diffuse large
B-Cell lymphomas. Bratisl Lek Listy. 2017; 118: 602-608.
- Ahmad AK, Hui P, Litkouhi B, et al. Institutional review of primary
non-hodgkin lymphoma of the female genital tract: a 33-year experience. Gynecol Cancer. 2014; 24: 1250-1255
- Stepniak A, Czuczwar P, Szkodziak P, Wozniakowska E, Wozniak S,
Paszkowski T. Primary ovarian Burkitt’s lymphoma: a rare oncological problem in gynaecology: a review of literature. Arch Gynecol
Obstet. 2017; 296: 653-660.
- Krol AD, le Cessie S, Snijder S, Kluin-Nelemans JC, Kluin PM, Noordijk EM. Primary extranodal non-Hodgkin’s lymphoma (NHL): the
impact of alternative definitions tested in the Comprehensive Cancer Centre West population-based NHL registry. Ann Oncol. 2003;
14: 131-139
- Fox H, Langley FA, Govan AD, Hill AS, Bennett MH. Malignant lymphoma presenting as an ovarian tumour: a clinicopathological analysis of 34 cases. Obstet Gynaecol. 1988; 95: 386-90.
- ZHAO Yan, DAI Lin, LU Xijing. Clinical analysis for 6 cases of primary
extra-nodal Non-Hodgkin lymphoma with manifestation as gynecologic neoplasm. Chin J Clin Obstet Gynecol. 2018; 19: 23-26.
- Hou Haixia, Li Guifen, Hou Suping. Clincal analysis of primary malignant lymphoma in the female genital system. Chinese Journal of
Cancer Prevention and Treatment. 2019. 26: 1479-1484.
- Wang J, Zeng L, Chen S, et al. Lymphoma of the female genital
tract: a clinicopatholngical analysis of 25 cases. Am J Transl Res.
2019; 11: 5800-5811.
- Ding Wenshuang, Li Xiubo. A case of ovarian primary with MYC
gene translocation diffuse large B-cell lymphoma. Journal of Shantou University School of Medicine. 2019; 3: 183-184.