Introduction
Germ cell tumors (GCTs) are the most common solid malignancy in men between the second and fourth decades of life. GCTs are found predominantly in the testis, but a non-despicable percentage of these tumors-5 to 10% - are Extragonadal in origin (EGCTs), with no identifiable testicular primary tumor [1,2]. They may be localized in almost every structure along the median axis of the body, arising particularly in the mediastinum and retroperitoneum [1,2]. When localized in the Central Nervous System (CNS) are generally called of Intracranial Germ Cell Tumors (IGCT) and may have many subtypes: teratoma; germinoma; embryonal carcinoma; yolk sac tumor; choriocarcinoma or mixed germ cell tumor [3].
IGCTs are a rare entity, most commonly found in younger patients - between the first and third decade of life, and their clinical presentation depends on the location and size of the tumor [3]. Although morphologically identical to their gonadal counterparts, they represent a heterogeneous group of tumors with very little current knowledge, especially in elderly patients [2]. We report a rare presentation of a nonseminomatous frontal lobe EGGCT in an elderly patient, with a subtle clinical presentation.
Case presentation
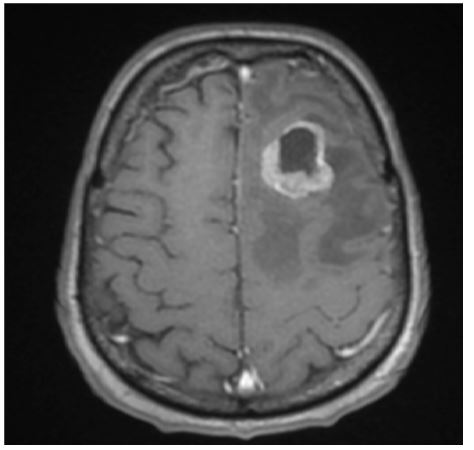
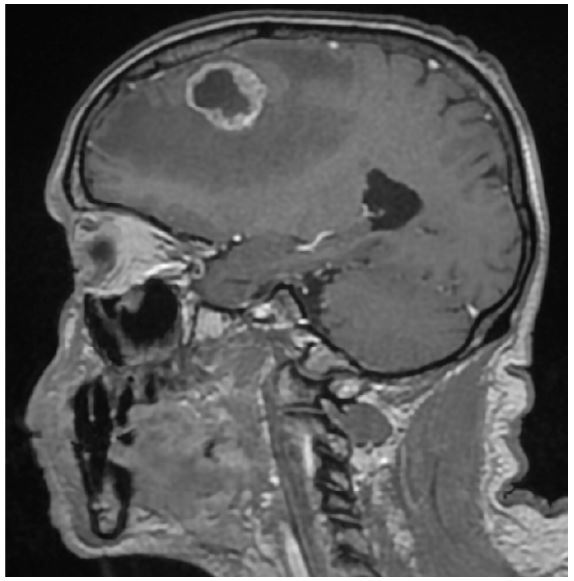
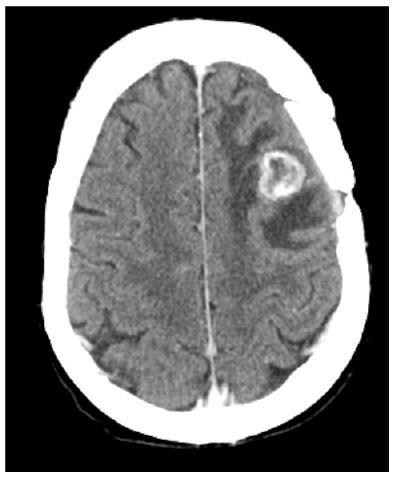
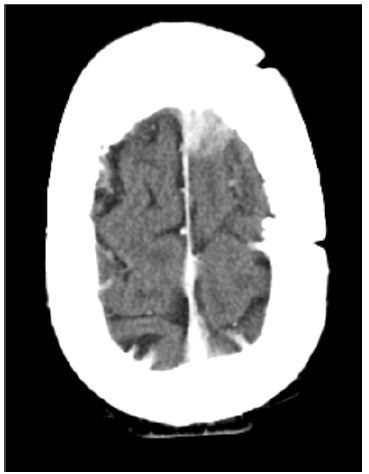
A 74-year-old patient presented to his family doctor with complaints of memory loss with one month of evolution. He denied any other symptoms like vomiting, headache or vision changes. His family doctor asked a Cranio-Encephalic Tomography (CE-CT) scan and a serum analysis with hormonal assessment. All blood parameters were normal and the CE-CT identified a frontal lesion with 3 x 2.3 cm, with no signs of hydrocephalus. He was referenced to the emergency department where he remained for further investigation and aa cranial MRI was performed (Figures 1,2).
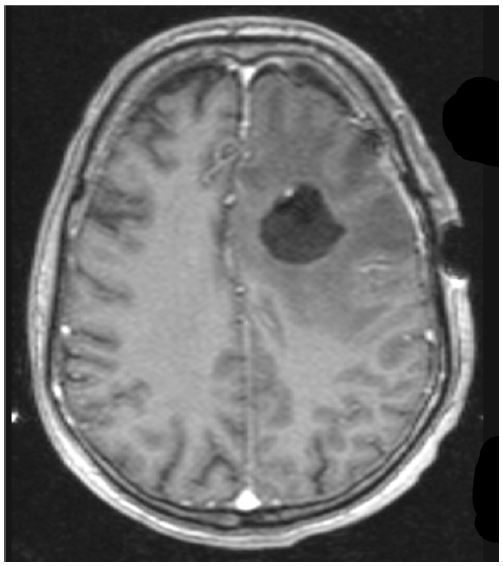
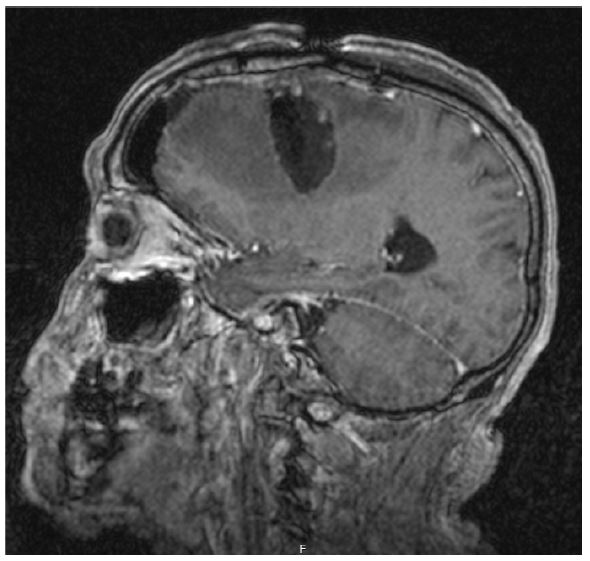
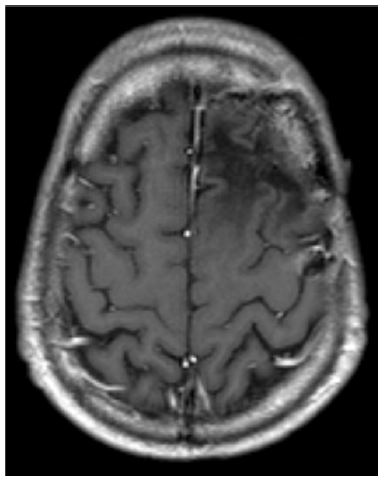
The patient was then admitted to the neurosurgery department, being submitted a few days later to an excisional biopsy, with macroscopically complete excision of the mass (Figures 3,4).The postoperative period was uneventful with partial recovery of memory. Histology revealed a lesion compatible with a germ cell tumor with areas of embryonal cell carcinoma. A new CT-scan, 5 months after surgery, identified two new frontal lesions with almost 1 centimeter each, one in the left centrum semiovale (Figure 5) and the other in the left frontal parasagittal area (Figure 6), with slightly smaller dimensions.
The patient was then sent to our center, where his case was discussed in a multidisciplinary meeting. Tumour markers and staging for other locations were negative, and the decision was to perform holo-cranial Radiotherapy (RT) in a total dose of 30Gy/10fr with a boost of 10Gy/5fr to lesions. After this treatment the cranial MRI showed complete resolution of the left frontal parasagittal area lesion (Figure 7) and stability of the lesion located in the left centrum semiovale. After careful evaluation and discussion, it was decided to maintain careful surveillance of the patient, without further treatment.
Investigations
At the initial investigation all blood parameters were normal, despite hemoglobin of 11.3 g/dL. A scrotal ultrasound was performed to rule out testis involvement, describing normal bilateral testis, without any suspicious masses or signs of burned-out testicular tumor. 107To rule out other tumor locations a body scan tomography and a Positron Emission Tomography (PET) scan were performed, with no evidence of distant metastasis. Tumor markers (LDH, βHCG and AFP) were also negative.
Outcome and follow up
After more than 18 months of follow-up, the patient remains stable and asymptomatic, with neuroimaging showing no progression of the lesions and body scans showing no metastization.
Discussion
iGCT are rare CNS tumours that mainly affect adolescents and young adults, with a peak incidence in the second decade of life [3]. According to the 2021 WHO classification4, iGCT are divided into germinoma (55%-65%) and non-germinomatous germ cell tumors (NGGCT) (35%-45%), which include embryonal carcinoma, yolk sac tumor, choriocarcinoma, and teratoma (mature, immature and teratoma with somatic-type malignancy) [1,4]. Mixed iGCTs contain two or more of the subtypes, including most often germinoma and teratoma [1]. It is assumed that EGCTs either develop from a malignant transformation of primordial germ cells that were misallocated during the first weeks of gestation, or from germ cells that have spread throughout the body during embryogenesis to fulfil different roles in immunological processes or distinct organ functions [2].
The most common EGCTs are found in the mediastinum followed by the retroperitoneum, with rare occurrence in the sacrococcygeal region and the CNS. IGCTs occur predominantly in midline locations of the CNS (mostly from pineal and suprasellar regions), with distinct clinical and biological dynamics from the most common EGCTs [2].
Clinical presentations of intracranial CGT are dependent on the location and size of the tumor, for example hydrocephalus and increased intracranial pressure in pineal tumors, or reduced visual acuity and hypothalamic-pituitary axis insufficiency in Suprasellar Tumors, but symptoms may be as subtle as in this case [1].
The diagnosis of iGCT is based on imaging, clinical signs, markers in serum and cerebrospinal fluid, and histology, being standard craniospinal MRI the primary imaging method for evaluating iGCTs [1]. The ideal management of iGCTs remains controversial [5]. Despite the fact that all GCT are radiosensitive and most are chemo sensitive, the relative role of surgery, Radiotherapy (RT) and Chemotherapy (CT) in the management of this type of lesions remains unsettled [6].
RT has been the cornerstone of the treatment of these patients, and the treatment volumes and dose vary according to the extent of the disease, histological subtypes, and the concomitant or previous response to chemotherapy [6]. The chemo sensitivity of iGCT is well documented [6]. Pre irradiation CT allows lowering the dose of RT, thus reducing the toxicity, what assumes particularly importance when it comes to younger patients [5,6]. iGCTs survival rates are reported over 90% [6]. Recent strategies have focused on reducing treatment to minimize long-term sequelae of treatment. The current standard treatment involves a combination of CT and RT, with surgery having a limited role [6,7].
Conclusion
In summary, this patient presented with a very rare clinical case of a frontal lobe localization of IGCT in an elderly man (74 years old), which justifies the importance of this case report. In this particular situation, and because of the age of the patient, we decided to omit CT, and the patient was only treated with RT, with very good response, proving again the high radio sensitivity of these tumors, and the importance of personalized treatment plans adjusted to our patient age and comorbidities.
Declarations
Conflicts of interest: No conficts of interest.
Funding sources: No funding sources.
Acknowledgments: I would like to express my gratitude to Dr Tiago Sousa who contributed to the design and drafting of the case report, Dr Arnaldo José Figueiredo and Dr Pedro Nunes who reviewed the case report text and its content, and Dr Ruben Miranda Cardoso and Dr Hermínio Tão, who selected and labeled the images presented in this case report. Additionally I would like to express my deep gratitude to the patient and his family, who kindly agreed on the publication of this case report.
References
- Packer RJ, Cohen BH, Cooney K. Intracranial germ cell tumors. Oncologist. 2000; 5(4): 312-20.
- Abdulfatah E, Brown NA, Davenport MS, Reichert ZR, Camelo-Piragua S, et al. Extragonadal germ cell tumors: A clinicopathologic study with emphasis on molecular features, clinical outcomes and associated secondary malignancies. Hum Pathol. 2024; 148: 41-50.
- Goodwin TL, Sainani K, Fisher PG. Incidence patterns of central nervous system germ cell tumors: A SEER Study. J Pediatr Hematol Oncol. 2009; 31(8): 541-4.
- Louis DN, Perry A, Wesseling P, Brat DJ, Cree IA, et al. The 2021 WHO Classification of Tumors of the Central Nervous System: a summary. Neuro Oncol. 2021; 23(8): 1231-1251. doi: 10.1093/neuonc/noab106.
- Frappaz D, Dhall G, Murray MJ, Goldman S, Faure Conter C, et al. EANO, SNO and Euracan consensus review on the current management and future development of intracranial germ cell tumors in adolescents and young adults. Neuro Oncol. 2022; 24(4): 516-27.
- Siddiqui BA, Zhang M, Pisters LL, Tu SM. Systemic therapy for primary and extragonadal germ cell tumors: prognosis and nuances of treatment. Transl Androl Urol. 2020; 9(Suppl 1): S56-S65.
- Murray MJ, Horan G, Lowis S, Nicholson JC. Highlights from the Third International Central Nervous System Germ Cell Tumour symposium: Laying the foundations for future consensus. Ecancermedicalscience. 2013; 7: 333.